Calcium Magnesium Vitamin D3 K2 Cycle Explained: The Ultimate Bone Strength, Recovery & Performance Guide
By Artemis_strength•May 26, 2026•11 min read
Calcium Magnesium Vitamin D3 K2 Cycle Explained: The Ultimate Bone Strength, Recovery & Performance Guide
Inside every rep of a heavy squat, every explosive sprint, and every mile logged on the pavement lies a quiet, coordinated biochemical symphony involving four unsung nutrients: calcium, magnesium, vitamin D3, and vitamin K2. Most athletes obsess over protein timing, creatine loading, and pre-workout stimulants, yet completely overlook the mineral-vitamin axis that literally holds their skeleton together and dictates how efficiently their muscles contract and recover. Osteoporosis is not just a grandmother’s disease; stress fractures, delayed union of micro-tears, and cramping are the performance-diminishing consequences of a dysfunctional calcium-magnesium-D3-K2 cycle. I have seen elite lifters with alarmingly low bone mineral density simply because they supplemented calcium without the directing power of K2, or took massive doses of vitamin D without magnesium to activate it.
This guide is not a superficial vitamin list. It is a deep dive into the interdependent metabolic relay where each player’s function depends on the presence and balance of the others. You will learn why you can swallow grams of calcium and still weaken your bones if K2 is absent, why vitamin D supplements might be inert without magnesium, and how the right ratios accelerate muscle recovery and protect your arteries from the silent plaque of calcium mismanagement. By the end, you will possess the supplementation blueprint, the food-sourcing strategy, and the critical reasoning to turn this quartet into one of the most powerful performance-enhancing, longevity-extending protocols available outside of prescription medicine.
The Biochemical Relay: Why These Four Nutrients Form an Unbreakable Cycle
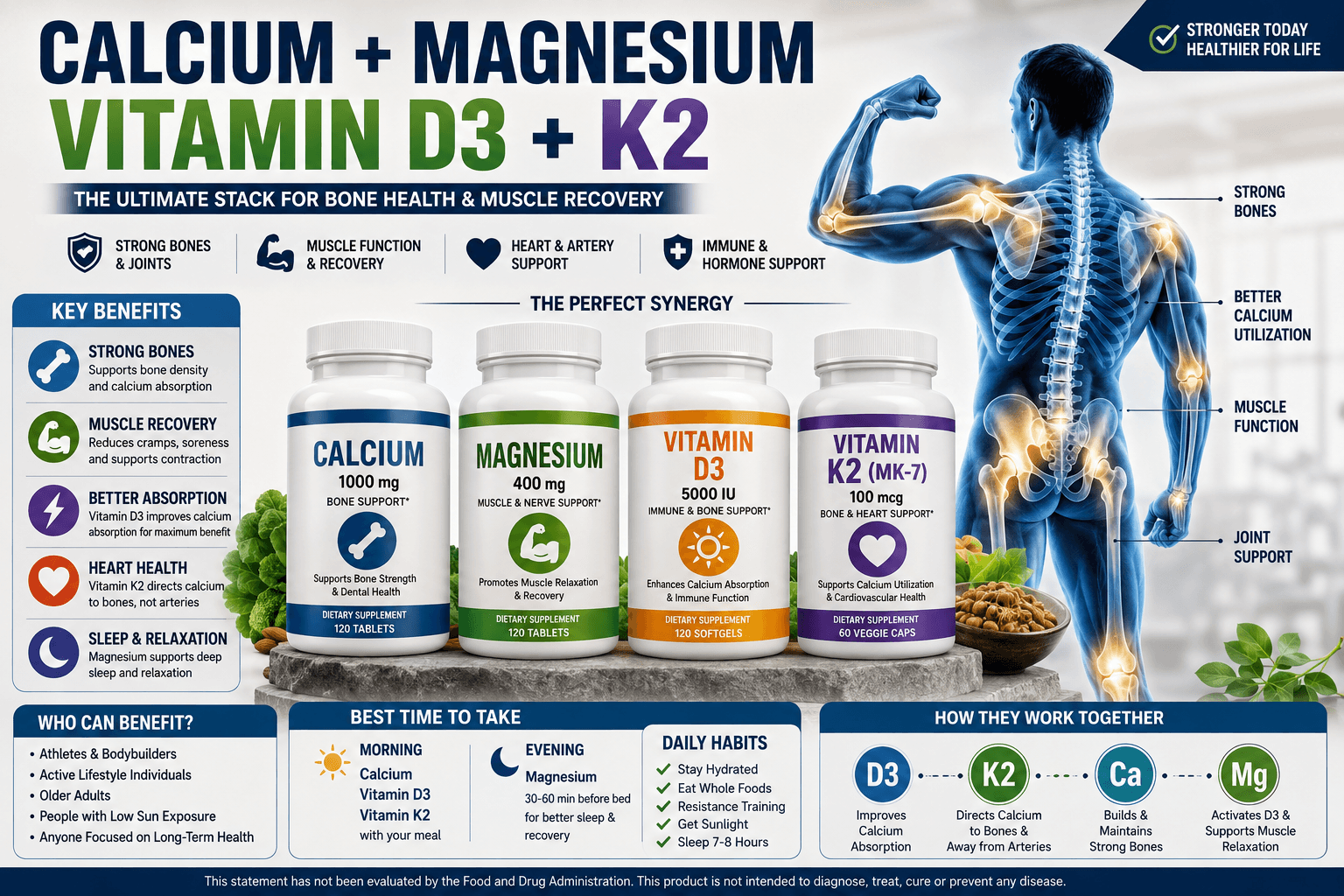
Calcium and magnesium are often framed as antagonists—calcium contracts muscles, magnesium relaxes them. But in the context of systemic health, they are dance partners in a tightly choreographed routine governed by two fat-soluble vitamins. Here’s the fundamental cycle: you ingest calcium; vitamin D3 dramatically increases its absorption from the gut into the bloodstream; but once in circulation, that calcium faces a critical fork in the road. Without adequate vitamin K2, the calcium that D3 mobilized can deposit in soft tissues—arteries, kidneys, joints—rather than being ushered into bone. [1] Magnesium is the stagehand that activates both vitamin D and K2. A deficiency in any single link causes the whole chain to malfunction, potentially turning a well-intentioned bone-support protocol into a cardiovascular risk.
Think of vitamin D3 as the project manager, calcium as the building material, magnesium as the tools and machinery, and vitamin K2 as the site foreman who directs exactly where the material gets placed. Remove the foreman, and you’ll get piles of bricks on the sidewalk (arterial calcification). Remove the tools, and the project halts (inactive vitamin D). This metaphor, while simplified, captures why isolated calcium supplementation has fallen out of favor in the most recent research, and why the quartet must be approached as a unified stack. Athletes who understand this cycle reduce injury risk, enhance power output through optimal nerve transmission, and build bone robust enough to withstand heavy eccentric loads.
Deep Dive: The Roles, Mechanisms, and Performance Implications
Calcium: More Than Just Bone Mass
Calcium is the most abundant mineral in the human body, with 99% stored in bone and teeth as hydroxyapatite. The remaining 1% circulates in blood, where it is so vital for nerve impulse transmission, muscle contraction, and blood clotting that the body will leach it from bone if dietary intake is insufficient. For athletes, ionized calcium is the trigger that allows actin and myosin filaments to slide over one another—without a rapid influx of calcium ions, no rep is possible. However, flooding the system with high-dose calcium without co-factors leads to hypercalcemia and ectopic calcification. A 2016 meta-analysis raised alarms that calcium monotherapy (without D3 and K2) could increase myocardial infarction risk by 31%, likely due to calcium deposition in coronary arteries. [2] So, the goal is not simply “more calcium,” but precisely directed, matrix-bound calcium deposition.
Key food sources include dairy, sardines with bones, fortified plant milks, and collard greens. Yet the absorption from spinach is poor due to oxalates. Supplement forms matter: calcium citrate is absorbed well on an empty stomach, while calcium carbonate requires stomach acid and is best taken with meals. The recommended dietary allowance (RDA) ranges from 1,000–1,200 mg per day, but high-performance athletes, especially those in energy deficit or amenorrheic female athletes, may need to be at the higher end while monitoring total intake from all sources.
Magnesium: The Master Activator
Magnesium is required as a cofactor for over 300 enzymatic reactions, including the conversion of vitamin D into its active hormonal form (calcitriol). All enzymes that metabolize vitamin D—the hydroxylases in the liver and kidneys—demand magnesium. A 2018 study in the Journal of the American Osteopathic Association found that people with low magnesium status could take large doses of vitamin D yet show no rise in serum 25-hydroxyvitamin D levels, effectively rendering the supplement useless. [3] For the athlete, magnesium’s role in ATP production (every ATP molecule must be bound to magnesium to be biologically active) makes it indispensable for muscular endurance and power output. Magnesium also opposes calcium’s excitatory effects at the neuromuscular junction, allowing muscle relaxation. A deficiency manifests as cramps, fasciculations, and poor sleep quality—all of which sabotage recovery.
Magnesium glycinate offers high bioavailability with minimal gastrointestinal distress, making it ideal for sleep and recovery support. Magnesium citrate is well-absorbed but can draw water into the bowel, which athletes prone to pre-competition nerves might want to avoid. Magnesium malate may reduce muscle pain via malic acid’s role in the Krebs cycle. The RDA is 310–420 mg but athletic populations sweating heavily in hot conditions lose substantial magnesium through sweat, pushing needs closer to 500–600 mg daily. Tracking total magnesium intake from food (almonds, spinach, black beans, pumpkin seeds) and supplementing to bridge the gap is a cornerstone of any serious performance nutrition plan.
Vitamin D3: The Solar Key to Absorption and Immunity
Vitamin D3 (cholecalciferol) is technically a steroid hormone precursor synthesized in the skin upon UVB exposure. It then undergoes hydroxylation in the liver to form 25-hydroxyvitamin D, the storage form, and in the kidneys to form 1,25-dihydroxyvitamin D, the active hormone. This active form upregulates calcium-binding proteins in the intestinal mucosa, increasing calcium absorption by up to 4-fold compared to passive diffusion. Without D3, you absorb only 10–15% of the calcium you consume. For bone health alone, this is devastating, but for athletes, D3’s influence on muscle protein synthesis, type II muscle fiber preservation, and immune resilience is equally critical. A 2020 study on collegiate athletes showed that those with sufficient vitamin D status (>30 ng/mL) had significantly lower rates of upper respiratory tract infections and faster recovery of muscle strength after eccentric damage. [4]
Optimal serum levels for performance sit at 40–60 ng/mL, yet most indoor athletes and northern-latitude dwellers are deficient. Supplementation with D3 (not D2) is superior for raising levels, typically at 2,000–5,000 IU daily as maintenance, with higher doses used under medical supervision for correction. Critically, vitamin D supplementation increases the body’s demand for magnesium, because the enzymes that activate D3 consume magnesium, and activated D3 enhances calcium absorption—creating a greater need for K2 to manage that calcium. This interdependence is the core of the cycle.
Vitamin K2: The Calcium Traffic Controller
Vitamin K2, specifically as menaquinone-7 (MK-7), is the missing link in most bone health protocols. It activates two critical proteins: osteocalcin, which binds calcium into the bone matrix, and matrix Gla protein (MGP), which inhibits calcium deposition in arteries and soft tissues. In essence, K2 simultaneously strengthens bone and decalcifies arteries. The Rotterdam Study demonstrated that high dietary intake of vitamin K2 was associated with a 52% reduction in severe aortic calcification risk and a 26% lower risk of coronary heart disease mortality. [5] For athletes, this translates to a vascular system that remains pliable and responsive under pressure, and bones that are dense enough to absorb ground reaction forces without stress fractures.
MK-7 from natto (fermented soy) is the star form due to its long half-life (about 3 days vs. MK-4’s 1–2 hours), allowing once-daily dosing. Typical doses for bone and cardiovascular support range from 90–180 mcg per day, although some protocols use up to 360 mcg under supervision. A word of caution: K2 can interfere with warfarin and other anticoagulants because those drugs work by blocking vitamin K recycling. Anyone on blood thinners must coordinate with their prescribing physician before adding K2.
The Vicious Cycle Without K2: How Calcium Ends Up in Your Arteries
To truly grasp the cycle, picture a well-intentioned person taking 1,000 mg of calcium plus 2,000 IU of vitamin D3 daily, but no magnesium or K2. The D3 effectively pulls more calcium from the gut into the bloodstream. However, due to low magnesium, the D3 may not be fully activated. Even if it is, the excess calcium has no active osteocalcin (because K2 is missing) to pull it into bone. Instead, it starts to deposit in the arterial media, creating a calcified plaque that increases arterial stiffness and pulse wave velocity. Simultaneously, magnesium deficiency leaves muscles unable to counter calcium’s contractile signal, leading to chronic tension and cramping. This scenario isn’t hypothetical—it’s a common pattern observed in patients presenting with both osteoporosis and atherosclerosis, a condition termed the “calcium paradox.” [6]
Breaking the cycle requires a shift in mindset: stop thinking of calcium as the primary actor and instead manage the system. The quartet approach ensures that calcium is absorbed only in amounts that can be properly directed into the skeleton and teeth, and that any excess is safely excreted rather than deposited. Athletes who integrate this concept not only preserve their long-term health but notice immediate functional improvements: fewer muscle cramps, better sleep, and a more consistent cardiac rhythm during intense intervals.
Recovery, Performance, and the Underrated Muscle-Bone Connection
Muscle and bone are not separate systems. They communicate mechanically through load and biochemically through myokines and osteokines. A strong muscle attached to a weak bone will eventually avulse the tendon or cause a fracture. Conversely, a well-mineralized bone with a weak muscle cannot move load effectively. The calcium-magnesium-D3-K2 cycle directly governs the mineralization of the collagen matrix laid down by osteoblasts, a process that accelerates after high-impact or resistance training as the bone adapts. Providing the full quartet post-workout—through a combination of a whole-food meal and targeted supplementation—gives the bone the raw materials to reinforce the specific lines of stress you just applied.
Furthermore, the cycle influences the hormonal environment of recovery. Vitamin D acts as a transcription factor for genes involved in muscle repair. Magnesium’s influence on GABA receptors improves deep sleep, during which growth hormone pulses and actual bone remodeling occur. K2’s ability to bind calcium into the matrix reduces the systemic inflammatory load that would otherwise be elevated after training. For masters athletes, who face age-related declines in bone density and vitamin D synthesis, this cycle becomes the foundation of longevity in sport. For younger athletes, it’s the difference between consistent, uninterrupted training blocks and repeated setbacks from stress reactions and soft-tissue injuries.
| Nutrient | Primary Role in the Cycle | Best Supplemental Form | Daily Target (Active Individuals) | Key Synergistic Note |
|---|---|---|---|---|
| Calcium | Bone matrix, nerve firing, muscle contraction | Calcium citrate or microcrystalline hydroxyapatite | 1,000–1,200 mg (diet + supplement) | Avoid exceeding 500 mg elemental per dose; requires K2 to reach bone |
| Magnesium | D3 activation, ATP production, muscle relaxation | Magnesium glycinate or malate | 400–600 mg (diet + supplement) | Take 2 hours apart from high-dose calcium to avoid competition for absorption |
| Vitamin D3 | Calcium absorption, muscle strength, immune modulation | Cholecalciferol (D3) with oil carrier | 2,000–5,000 IU (maintenance; adjust via blood test) | Must be taken with dietary fat; increases demand for magnesium |
| Vitamin K2 (MK-7) | Directs calcium to bone, prevents arterial calcification | Menaquinone-7 (MK-7) from natto extract | 100–180 mcg | Fat-soluble; take with the same meal as D3 and dietary fat |
Supplement Quality Protocols: Timing, Ratios, and Third-Party Testing
Administering the cycle optimally requires more than just opening a bottle. The timing of doses relative to each other and to meals influences both efficacy and safety. A high dose of calcium can temporarily saturate transport mechanisms, so splitting calcium into two 500 mg doses improves absorption. Magnesium is best taken in the evening due to its calming effect, but a second dose post-training can replace sweat losses. Vitamin D3 and K2 are both fat-soluble and should be consumed with the fattiest meal of the day—typically lunch or dinner—to enhance absorption by up to 50%. [7] I recommend keeping D3 and K2 in the same capsule or taking them together, as they function as a bonded pair in the cycle.
Not all supplements are created equal. Look for products certified by NSF Certified for Sport, Informed-Sport, or USP. This ensures that the label matches the content and that no banned substances contaminate the batch. For the K2 component, verify the form on the supplement facts panel: it should say “menaquinone-7 (MK-7)” and ideally specify the source as “from natto.” Many cheap supplements use MK-4 at doses too small to have any systemic effect on osteocalcin activation, essentially wasting your money. For athletes in aesthetic sports with strict weight classes, calcium and magnesium should be counted in your total mineral intake if tracking closely, but they don’t impact calorie or macro counts. Blood testing for 25-hydroxyvitamin D twice yearly (aiming for 40–60 ng/mL) and a red blood cell magnesium test provide the empirical data to fine-tune doses beyond generic recommendations.
Optimization Tip: On heavy lifting days, take your magnesium glycinate post-workout with a carbohydrate-protein shake. The carbohydrate spike increases insulin, which drives magnesium into muscle cells where it can assist with energy metabolism and relaxation, and the glycine aids post-exercise neural recovery.
Food-First Synergy: Building the Cycle from Your Plate
Supplementation closes gaps, but the foundation must be dietary. A diet rich in leafy greens provides a calcium-magnesium base; wild-caught salmon offers both D3 and calcium (from edible bones in canned salmon); natto, a traditional Japanese fermented soybean dish, is the richest natural source of vitamin K2 MK-7 by an enormous margin—a single tablespoon provides over 350 mcg. [8] Integrating natto into an athlete’s diet can be challenging due to its acquired taste and texture, but mixing it into rice bowls with spicy mustard and avocado masks the slime while adding healthy fats that boost K2 absorption. For those who cannot tolerate natto, aged cheeses like Gouda and Brie contain modest amounts of MK-7, though far less than natto.
A sample day that hits all four nutrients without a single pill might look like this: breakfast of scrambled eggs (D3 if pasture-raised), sautéed spinach and mushrooms (calcium, magnesium), topped with fermented kimchi or a side of natto (K2). Lunch of canned wild salmon with bones, a quinoa and kale salad dressed in olive oil. Post-workout smoothie with yogurt, frozen kale, and a handful of pumpkin seeds. While this provides a solid base, most individuals—especially those with indoor lifestyles, high sweat rates, or limited sun exposure—will still need a maintenance supplement stack to consistently hit optimal serum levels. The goal is to have the diet reduce the supplement burden, not replace it entirely.
Myths That Break the Cycle
Myth 1: “I Drink Milk Daily, So My Bones Are Fine”
Milk provides calcium and often is fortified with D3, but it contains zero K2 (unless from grass-fed sources with some MK-4, but minimal MK-7). Without K2, the calcium you absorb thanks to D3 may not be directed into bone. Additionally, many people stop consuming milk in their 20s, just as bone accrual peaks. Bone is a living tissue requiring daily investment; past consumption doesn’t inoculate you against future loss.
Myth 2: “Magnesium Isn’t Important if I Don’t Get Cramps”
Absence of cramps is a poor gauge of magnesium status. The body tightly regulates serum magnesium at the expense of tissue stores. You can have normal blood magnesium but depleted muscle and bone reserves, subtly impairing D3 activation and ATP synthesis. By the time cramps appear, you are often severely depleted. A 2021 review found that subclinical magnesium deficiency affects up to 50% of the population and is linked to chronic inflammation and reduced athletic performance. [9]
Myth 3: “Vitamin D Toxicity Is Easy to Reach”
While vitamin D is fat-soluble and can accumulate, toxicity (hypercalcemia, kidney stones) is extremely rare and usually requires doses over 10,000–20,000 IU daily for many months, coupled with inadequate magnesium and K2 intake. The inclusion of magnesium and K2 in the cycle is precisely what mitigates the risk of toxicity by ensuring calcium stays in bone and D3 is properly metabolized. Sensible supplementation within the 2,000–5,000 IU range is safe for virtually all adults.
Practical 4-Step Protocol to Activate the Cycle for Life
- Test, Don’t Guess: Order a 25-hydroxyvitamin D blood test and a red blood cell (RBC) magnesium test. If RBC magnesium is below 5.5 mg/dL, prioritize magnesium repletion for 6–8 weeks before ramping D3 aggressively. Target vitamin D levels of 40–60 ng/mL.
- Structure Your Stack: With your largest meal containing fat, take vitamin D3 (based on test results) and vitamin K2 MK-7 (100–180 mcg). If your diet provides less than 1,000 mg calcium, add 500 mg calcium citrate in the morning and another 500 mg in the evening. Take magnesium glycinate (200–300 mg) in the evening, and optionally another 100–200 mg post-training.
- Prioritize Bone-Loading Exercise: The cycle provides the materials, but mechanotransduction provides the blueprint. Perform heavy resistance training that loads the spine and hips—deadlifts, squats, overhead presses—at least twice per week. Impact-based activities like jumping jacks, box jumps, or sprinting send piezoelectric signals that direct osteocalcin-bound calcium exactly where it is needed.
- Reassess Every 6 Months: Recheck vitamin D levels, and also request a serum calcium and parathyroid hormone (PTH) test. If PTH is elevated despite adequate vitamin D and calcium intake, you may need to adjust your K2 dose or investigate magnesium status further. This feedback loop turns supplementation from a static habit into a dynamic precision tool.
Critical Note: If you have kidney disease, sarcoidosis, or are on anticoagulants (especially warfarin), the calcium-D3-K2 protocol can be dangerous. Vitamin K2 directly opposes warfarin’s mechanism, and hypercalcemia risk is higher with certain conditions. Always consult your nephrologist or cardiologist before integrating these nutrients.
FAQ: Your Cycle Questions Answered
Can I take all four nutrients in a single combined supplement?
Yes, many all-in-one bone formulas now include calcium, magnesium, D3, and K2. The convenience is appealing, but scrutinize the forms and doses. Many use cheap magnesium oxide (poorly absorbed) and minimal MK-7 (often 45 mcg or less). If the product meets your target doses with bioavailable forms, it’s a reasonable option. However, splitting magnesium into evening and post-workout doses separately from calcium may provide superior results for athletes, which a single pill cannot accommodate.
Does the cycle influence testosterone or anabolic hormones?
Indirectly, yes. Magnesium and vitamin D3 are both correlated with higher free testosterone levels and lower sex hormone-binding globulin (SHBG) in deficient individuals. Zinc is another mineral player in testosterone, but magnesium’s role in sleep and vitamin D’s steroid-like receptor activity create an environment supportive of anabolic pathways. [10] While the cycle is not a replacement for proper nutrition and training, correcting deficiencies can remove a hormonal bottleneck.
Will taking these supplements improve my sleep and performance the next day?
Magnesium glycinate, especially at 200–400 mg before bed, can significantly improve sleep onset and depth because glycine lowers core body temperature and magnesium activates the parasympathetic nervous system. Better sleep directly translates to faster reaction times, better motor learning consolidation, and higher growth hormone output. Athletes often report less muscle soreness and a more refreshed feeling upon waking after 2–3 weeks of consistent magnesium supplementation within the cycle.
How long until I see improvements in bone density scans?
Bone turnover is slow. A DEXA scan typically requires 12–24 months to reflect meaningful changes in bone mineral density. However, markers of bone resorption (NTX, CTX) in urine or blood can shift within 3–6 months when the cycle is optimized. If you are using this protocol to prevent stress fractures or aid healing, focus on the functional outcomes—pain reduction, training tolerance—rather than waiting for a DEXA change.
Conclusion: Cement Your Foundation, Elevate Your Performance
The calcium-magnesium-vitamin D3-K2 cycle is not a supplemental afterthought—it is the very substrate of your body’s structural integrity. Every time you load your spine with a barbell, every time you absorb the shock of a running stride, your bones and arteries rely on this quartet to handle the stress without failure. By understanding the cycle, you move from blind supplementation to a targeted, intelligent strategy that uses each nutrient for its unique contribution while respecting their mutual dependence. You prevent the calcium paradox, you activate your vitamin D, you relax your muscles, and you build a skeleton that can carry you through decades of athletic pursuit.
Take action now. Open your supplement cabinet and read the labels. If you see calcium without K2, add it. If your magnesium is oxide, replace it. Schedule that 25-hydroxyvitamin D blood test you’ve been putting off. Share this guide with your training partner, because bone health is silent until it breaks, and by then, a season or a lifetime of progress can be lost. Commit to the cycle, and you commit to a foundation that turns every rep, every sprint, and every workout into a deposit of strength that accumulates for years. Your skeleton is the scaffold of your strength—invest in it with the precision it deserves.
References
- Schurgers, L. J. et al. "Matrix Gla-protein: the calcification inhibitor in need of vitamin K." Thrombosis and Haemostasis (2008).
- Bolland, M. J. et al. "Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis." BMJ (2011).
- Dai, Q. et al. "Magnesium status and the metabolism of vitamin D." Journal of the American Osteopathic Association (2018).
- He, C. S. et al. "Influence of vitamin D status on respiratory infection incidence and immune function during 4 months of winter training in endurance athletes." Exercise Immunology Review (2013).
- Geleijnse, J. M. et al. "Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study." Journal of Nutrition (2004).
- Reid, I. R. "Calcium and vitamin D: To supplement or not?" Cleveland Clinic Journal of Medicine (2018).
- Mulligan, G. B. & Licata, A. "Taking vitamin D with the largest meal improves absorption and results in higher serum levels of 25-hydroxyvitamin D." Journal of Bone and Mineral Research (2010).
- Kaneki, M. et al. "Japanese fermented soybean food as the major determinant of the large geographic difference in circulating levels of vitamin K2: possible implications for hip-fracture risk." Nutrition (2001).
- Nielsen, F. H. "Magnesium deficiency and increased inflammation: current perspectives." Journal of Inflammation Research (2018).
- Pilz, S. et al. "Effect of vitamin D supplementation on testosterone levels in men." Hormone and Metabolic Research (2011).
Share
