Best Peptides for Fat Loss: Complete Guide to AOD 9604, Cagrilintide, Semaglutide, Tirzepatide, Retatrutide, Tesamorelin, Ipamorelin & Frag 176-191
By Artemis_strength•May 30, 2026•8 min read
Best Peptides for Fat Loss: Complete Guide to AOD 9604, Cagrilintide, Semaglutide, Tirzepatide, Retatrutide, Tesamorelin, Ipamorelin & Frag 176-191
Medical Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice. The peptides discussed are primarily research chemicals or prescription medications, many of which are not FDA-approved for fat loss or bodybuilding purposes. Use of these compounds without medical supervision may pose serious health risks including hormonal disruption, pancreatitis, hypoglycemia, and unknown long-term effects. Always consult a qualified healthcare professional before considering any peptide therapy. Information presented is based on available research as of 2026.

The quest for a leaner physique has moved far beyond crash diets and endless cardio. Today, a new frontier has emerged: peptides—short chains of amino acids that signal the body to burn fat, curb appetite, and optimize metabolism. But the landscape is crowded, confusing, and often dangerous if navigated without a map. From the well-known GLP-1 agonists like semaglutide to targeted fat-burning fragments like AOD 9604 and Frag 176-191, each peptide works through distinct biological pathways. Some shrink visceral fat, others suppress hunger, and a few attempt to do both. As a sports nutritionist and performance researcher, I’ve seen these compounds transform stubborn fat loss cases, but I’ve also witnessed the consequences of misuse. This guide is your definitive, evidence-based compass.
We will dissect eight key peptides—AOD 9604, Cagrilintide, Semaglutide, Tirzepatide, Retatrutide, Tesamorelin, Ipamorelin, and Frag 176-191—examining their mechanisms, fat loss efficacy, clinical trial data, and safety profiles. You’ll learn which peptides target subcutaneous belly fat, which shrink visceral adipose tissue, and which suppress appetite so powerfully they rewrite the brain’s reward response to food. Beyond the science, we’ll provide practical protocols, stacking considerations, and critical nutrition and training strategies to ensure that the weight you lose is fat, not muscle. Whether you’re a biohacker, an athlete struggling with a final fat-loss plateau, or simply curious about the future of obesity treatment, this guide will arm you with the knowledge to think critically and act safely.
How Peptides Enable Fat Loss: The Core Mechanisms
Before diving into individual compounds, it is essential to understand the physiological levers that fat loss peptides pull. Adipose tissue is not a passive storage depot; it is an endocrine organ responding to hormonal and neural signals. Peptides exploit these signaling pathways in highly specific ways:
- Appetite Suppression and Satiety Enhancement: GLP-1 receptor agonists slow gastric emptying and act on hypothalamic feeding centers to reduce hunger and increase fullness. This reduces caloric intake effortlessly.
- Lipolysis Activation: Some peptides trigger the breakdown of stored triglycerides into free fatty acids, particularly in stubborn fat depots that are resistant to catecholamines.
- Growth Hormone (GH) Pulsatility Augmentation: GH secretagogues like Ipamorelin increase endogenous GH release, which promotes lipolysis and fat oxidation while preserving lean mass.
- Visceral Adipose Tissue Reduction: Tesamorelin specifically targets visceral fat through the GH axis, reducing the inflammatory abdominal fat linked to metabolic disease.
- Metabolic Rate and Substrate Shifting: Certain compounds upregulate mitochondrial uncoupling or shift the body’s fuel preference toward fatty acids.
Comprehensive Comparison of Leading Fat Loss Peptides
| Peptide | Primary Mechanism | Primary Fat Target | Average Reported Fat Loss | Route/Frequency |
|---|---|---|---|---|
| AOD 9604 | GH receptor fragment, lipolysis stimulation | Subcutaneous (stubborn belly fat) | Modest (1-3 kg over 12 weeks) [1] | Injection; 1-2x daily |
| Cagrilintide | Amylin analog, delayed gastric emptying, satiety | Overall body fat via appetite reduction | Synergistic when combined with semaglutide [2] | Weekly injection |
| Semaglutide | GLP-1 receptor agonist | Overall adiposity, visceral | ~15% body weight loss (STEP trials) [3] | Weekly injection |
| Tirzepatide | Dual GIP/GLP-1 agonist | Overall, profound visceral | Up to 21% body weight loss (SURMOUNT) [4] | Weekly injection |
| Retatrutide | Triple agonist (GIP, GLP-1, glucagon) | Overall, highly potent metabolic reset | Up to 24% body weight loss (Phase 2) [5] | Weekly injection |
| Tesamorelin | GHRH analog, increases GH/IGF-1 | Visceral adipose tissue (VAT) | ~15% VAT reduction (FDA-approved for HIV lipodystrophy) [6] | Daily injection |
| Ipamorelin | Ghrelin receptor agonist, GH pulse | Indirect fat loss through GH | Mild; best stacked with CJC-1295 | 1-3x daily injection |
| Frag 176-191 | hGH fragment, lipolysis without IGF-1 | Subcutaneous fat, especially abdomen | Variable, often stacked with AOD 9604 | 2-3x daily injection |
AOD 9604: The Targeted Belly Fat Fragment

AOD 9604 is a modified fragment of human growth hormone (hGH), encompassing amino acids 177-191 with an added tyrosine. It was originally developed to capture the fat-reducing properties of hGH without the muscle growth or blood sugar side effects. Mechanistically, AOD 9604 mimics the way natural GH binds to adipocytes, activating hormone-sensitive lipase to release stored fatty acids. Crucially, it does not increase insulin-like growth factor 1 (IGF-1) or cell proliferation, which has made it particularly attractive for those seeking fat loss without anabolic or mitogenic risks. [7]
Research, including early-phase clinical trials, demonstrated that AOD 9604 reduced up to 1.5 kg of body weight over 12 weeks in obese subjects when combined with a caloric deficit, with a favorable safety profile. However, the magnitude of fat loss is modest compared to GLP-1 agonists. It appears to work best on stubborn subcutaneous fat that resists diet and exercise—think love handles and lower belly. Many fitness users stack AOD 9604 with Frag 176-191 or a GLP-1 agonist for enhanced lipolysis. Typical protocol involves 250-500 mcg injected once or twice daily, often fasted or before cardio. Side effects are generally mild, including transient injection-site reactions or mild nausea. [8]
Frag 176-191: The Original Growth Hormone Fat Loss Fragment

Fragment 176-191 is the C-terminal portion of the hGH molecule, isolated to retain the lipid-metabolizing effects while eliminating carbohydrate-handling and growth-promoting properties. It accomplishes this by binding the GH receptor and triggering the cascade that activates lipolysis, but without the conformational change that induces IGF-1 production. The result is a peptide that some research indicates can more potently stimulate fat oxidation than intact GH, at least in vitro. [9]
In practice, Frag 176-191 is typically dosed at 250-500 mcg, administered 2-3 times daily on an empty stomach, as circulating nutrients blunt its action. Users often combine it with fasted cardio to maximize free fatty acid release. However, the peptide has no FDA approval, and human data is extremely limited. Anecdotally, it is used for targeted abdominal fat loss, but the results are inconsistent and highly dependent on diet and exercise. Common side effects include injection-site irritation and minor water retention.
The GLP-1 Revolution: Semaglutide, Tirzepatide, and Retatrutide


No discussion of fat loss peptides is complete without a deep dive into the incretin mimetics that have reshaped obesity medicine. These drugs are manufactured peptides, taken weekly, that fundamentally alter the brain’s appetite regulation and the gut’s nutrient handling.
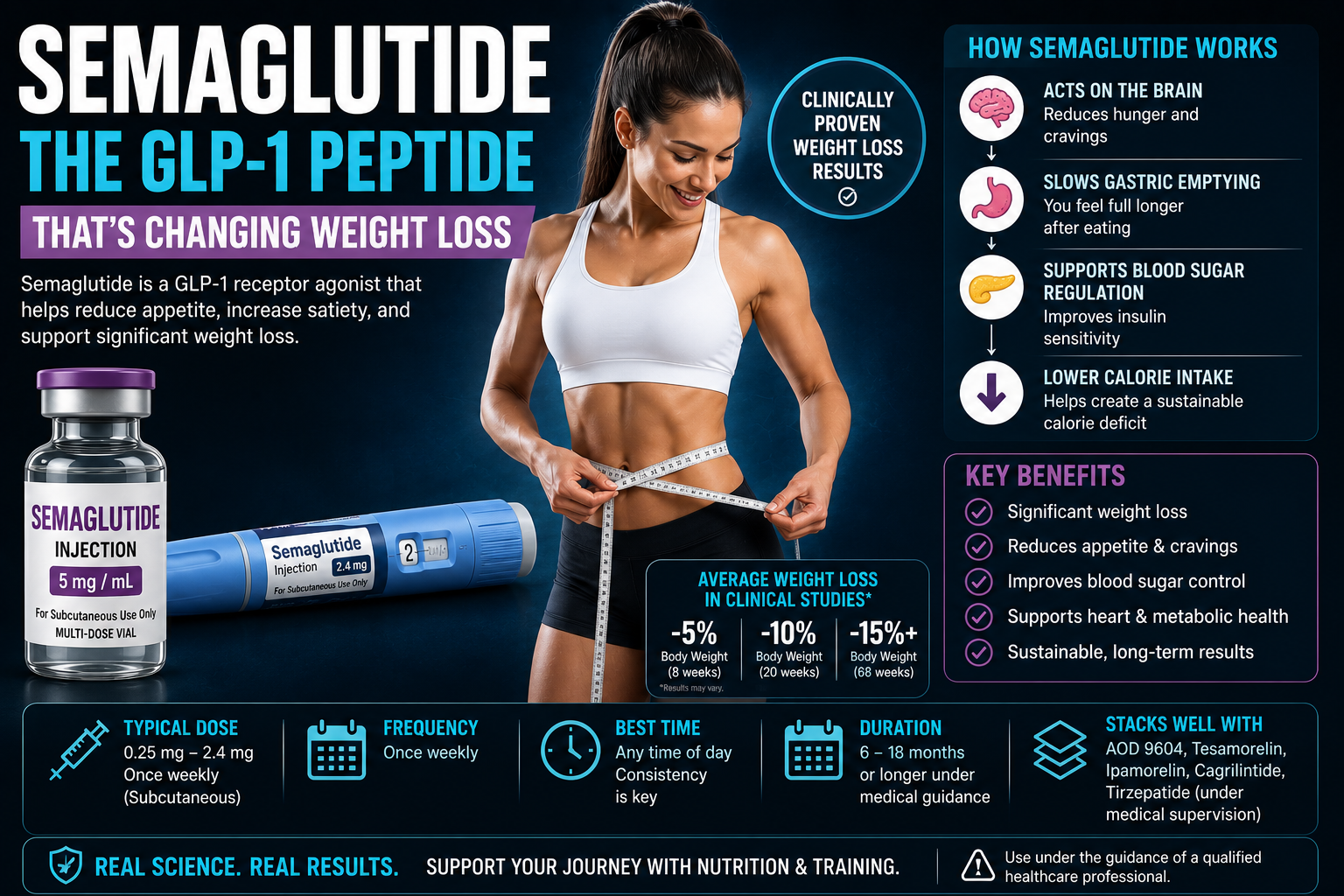
Semaglutide (Wegovy, Ozempic)
Semaglutide is a GLP-1 receptor agonist with 94% sequence homology to human GLP-1. It slows gastric emptying, promotes insulin secretion in a glucose-dependent manner, and activates POMC neurons in the hypothalamus to suppress appetite. The STEP clinical trials demonstrated an average 14.9% reduction in body weight over 68 weeks, with one-third of participants losing over 20% of initial body weight. [3] For fat loss athletes, semaglutide is a potent tool, but the rapid weight loss can include significant lean mass unless protein intake is kept high (1.6-2.4 g/kg) and resistance training is maintained. Common side effects include nausea, vomiting, and diarrhea, most prominent during dose titration.
Tirzepatide (Zepbound, Mounjaro)
Tirzepatide is a first-in-class dual agonist of both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors. The GIP component enhances the metabolic benefits, improving insulin sensitivity and possibly reducing the GI side effects compared to pure GLP-1 agonism. The SURMOUNT-1 trial recorded a staggering 20.9% mean weight loss at 72 weeks. [4] For the physically active individual, tirzepatide’s ability to improve fat oxidation and preserve muscle mass may be superior to semaglutide, though more direct comparison studies are underway.
Retatrutide
Retatrutide adds a third receptor: the glucagon receptor, alongside GIP and GLP-1. Glucagon agonism increases energy expenditure and hepatic fat oxidation, creating a triple threat against adipose tissue. Phase 2 data presented at the American Diabetes Association showed up to 24% weight loss at 48 weeks, approaching bariatric surgery territory. [5] Retatrutide may also more effectively reduce liver fat, making it a candidate for those with NAFLD. However, the glucagon component can raise blood glucose, so monitoring is critical. This peptide is still experimental, and its risk profile is less characterized.
Cagrilintide: The Amylin Analog That Supercharges Satiety
Cagrilintide is a long-acting analog of amylin, a hormone co-secreted with insulin from pancreatic beta cells. Amylin complements insulin by slowing gastric emptying, suppressing post-meal glucagon, and signaling satiety through the area postrema. Cagrilintide has been studied in combination with semaglutide as a fixed-dose therapy, with promising results: the combination amplified weight loss compared to semaglutide alone, while preserving lean mass better than monotherapy. [2] This synergy makes Cagrilintide an intriguing piece of the fat loss puzzle, especially for individuals who experience hunger breakthrough on GLP-1 agonists alone. Currently, it remains in clinical development, and its off-label use carries unknown risks.
Tesamorelin: The Visceral Fat Specialist
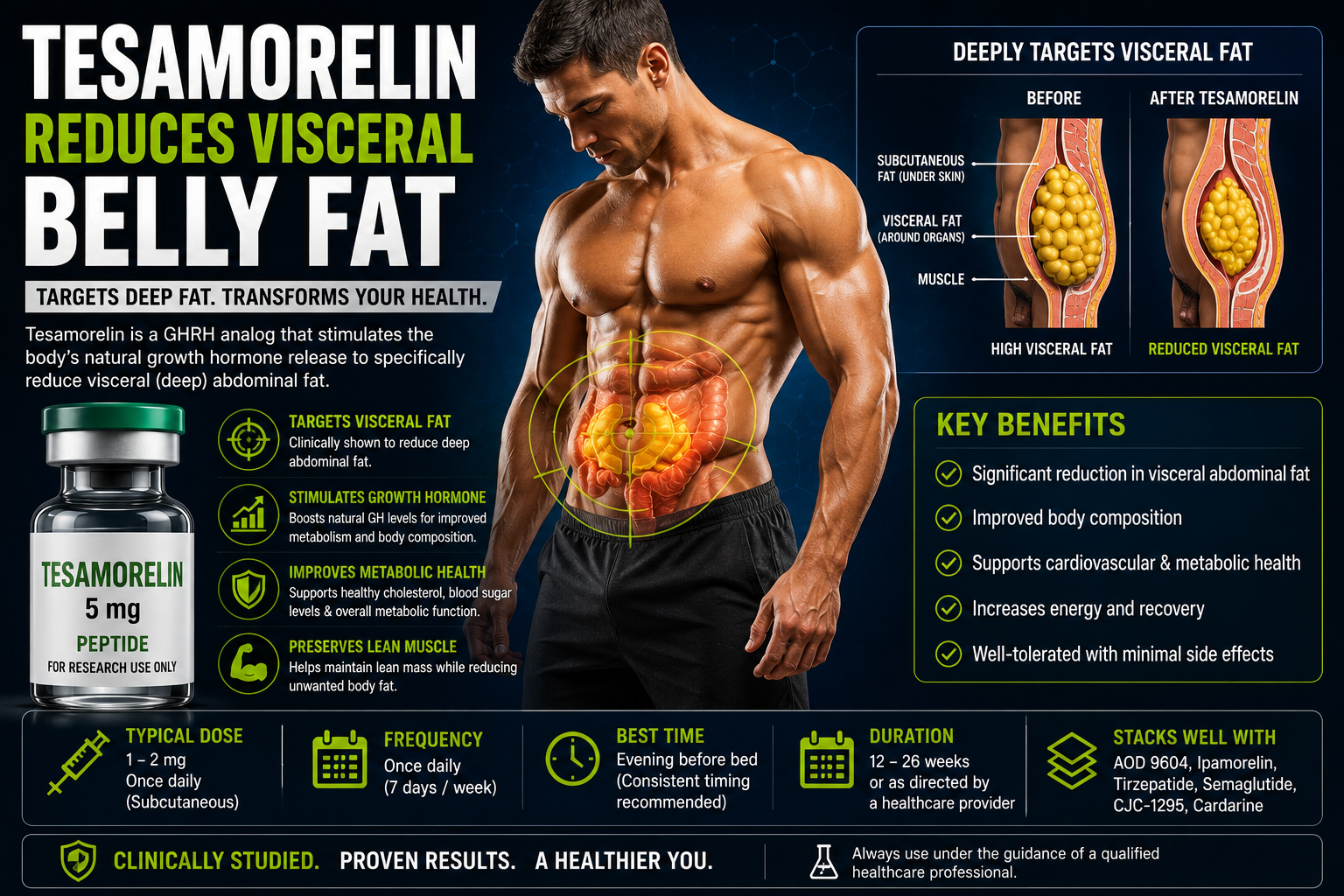
Tesamorelin is a synthetic growth hormone-releasing hormone (GHRH) analog that is FDA-approved for the reduction of excess abdominal visceral fat in HIV-positive patients with lipodystrophy. It stimulates the pituitary to produce and release growth hormone, which then targets the deep visceral adipose tissue that wraps around organs and drives metabolic dysfunction. In clinical trials, tesamorelin reduced visceral adipose tissue by approximately 15% over 26 weeks, without significantly altering subcutaneous fat. [6] This specificity is unique among fat loss peptides.
For non-HIV individuals, tesamorelin is used off-label to reduce visceral fat, improve lipid profiles, and enhance recovery. Typical doses are 2 mg injected once daily. Side effects mirror those of GH elevation: joint pain, fluid retention, and potential insulin resistance with prolonged use. Because it acts through the GH axis, tesamorelin is often stacked with Ipamorelin or combined with CJC-1295 for sustained GH pulses. It does not directly suppress appetite, making it complementary to the GLP-1 agonists that do.
Ipamorelin: The Lean Mass Preserving GH Secretagogue
Ipamorelin is a selective ghrelin receptor agonist and growth hormone secretagogue. Unlike GHRP-6 or GHRP-2, it produces minimal appetite stimulation, making it suitable for fat loss phases. The increased GH pulses promote lipolysis while preserving lean mass, which is critical during a caloric deficit. While Ipamorelin alone has modest fat loss effects, when combined with CJC-1295 (a GHRH analog), it creates a synergistic GH elevation that enhances body recomposition. [10] A typical protocol involves 100-300 mcg of each, injected 1-3 times daily on an empty stomach.
Coach’s Insight: Ipamorelin’s real value in a fat loss stack is not dramatic weight loss, but the preservation of muscle and improvement in sleep quality and recovery, which allow you to train harder and maintain metabolic rate during a deficit. Pair it with a GLP-1 agonist for appetite control and a targeted fragment for stubborn fat.
Designing a Fat Loss Peptide Protocol: Stacking, Timing, and Safety
Combining peptides requires a deep understanding of their mechanisms and potential interactions. A poorly planned stack can blunt effects or amplify side effects. Below are three example protocols based on current community knowledge and clinical data. These are not prescriptions; they are illustrations of how concepts might be integrated under hypothetical medical supervision.
| Goal | Peptides Involved | Rationale | Notes |
|---|---|---|---|
| Aggressive appetite control + metabolic reset | Semaglutide (or Tirzepatide) + Cagrilintide | GLP-1 agonism plus amylin satiety; reduces calorie intake profoundly | Requires aggressive protein and resistance training to prevent muscle loss; start low, titrate slow |
| Visceral fat reduction + lean mass preservation | Tesamorelin + Ipamorelin/CJC-1295 | GHRH drives GH for visceral loss; secretagogues sustain GH pulsatility and support muscle | Monitor glucose; ensure adequate sleep; may cause water retention initially |
| Stubborn subcutaneous fat + final cutting phase | AOD 9604 + Frag 176-191 + Ipamorelin | Direct lipolysis in belly fat; GH secretagogue preserves muscle and enhances recovery | Requires fasted cardio and precise diet; results are gradual; injection frequency high |
Critical Safety Reminder: All injectable peptides carry risks: contamination, infection, and inaccurate dosing from non-pharmaceutical sources. Always source from a reputable compounding pharmacy or clinical trial. Never share needles. Regular blood work—including fasting glucose, HbA1c, amylase, lipase, liver enzymes, and lipid panel—is mandatory for anyone using these compounds.
Nutrition and Training: The Non-Negotiables for Peptide-Assisted Fat Loss
No peptide can outwork a poor diet. In fact, the synergy between nutrition and these compounds is what determines success. The key principles include:
- Protein Priority: Maintain 1.6-2.2 g/kg protein to preserve lean mass, especially when appetite is suppressed by GLP-1 agonists.
- Strength Training: Resistance exercise is non-negotiable to direct the body toward fat oxidation and away from muscle catabolism.
- Fasted Cardio with Targeted Peptides: When using AOD 9604 or Frag 176-191, performing low-intensity cardio in a fasted state may amplify lipolysis in stubborn fat areas.
- Hydration and Electrolytes: GLP-1 agonists can cause dehydration due to nausea and reduced thirst; electrolytes are crucial.
- Micronutrient Support: A high-quality multivitamin, omega-3s, and magnesium support metabolic health and mitigate some side effects.
Myths That Distort the Fat Loss Peptide Landscape
Myth 1: “Peptides burn fat without any effort.”
Peptides alter physiology, but they do not replace the laws of thermodynamics. A caloric deficit is still required; peptides make it easier to sustain. The weight loss comes from the deficit, not from the peptide directly burning calories, except for very modest thermogenic effects.
Myth 2: “Frag 176-191 and AOD 9604 are just as powerful as semaglutide.”
These fragments can help mobilize stubborn fat but do not produce the double-digit percentage weight losses of GLP-1 agonists. They are more suited for fine-tuning body composition in already-lean individuals.
Myth 3: “You can take GLP-1 peptides for a quick cut and stop.”
Discontinuation without a maintenance plan leads to weight regain in a majority of cases. These are long-term metabolic therapies, not temporary fixes.
Myth 4: “Natural peptides like Ipamorelin have no side effects.”
Ipamorelin can elevate prolactin and cortisol at high doses, and any GH secretagogue can contribute to insulin resistance over time. Monitoring is required.
Frequently Asked Questions
Which peptide is best for losing belly fat specifically?
For visceral fat, Tesamorelin is the most targeted. For subcutaneous belly fat, AOD 9604 and Frag 176-191 are popular, but their effects are modest. Overall, GLP-1 agonists like Tirzepatide reduce both depots effectively.
Can I stack GLP-1 agonists with growth hormone peptides?
Yes, under supervision. The combination can control appetite while preserving muscle through GH pathways. However, glucose monitoring is essential, as GH can induce insulin resistance while GLP-1s enhance insulin sensitivity; the interaction is complex.
Do these peptides affect muscle mass?
GH secretagogues like Ipamorelin and Tesamorelin can help preserve or even slightly increase lean mass. GLP-1 agonists alone often lead to some lean mass loss if protein and training are insufficient. Always prioritize protein and resistance exercise.
What are the risks of buying peptides online?
Risks include receiving counterfeit, underdosed, or contaminated products. There is no regulatory oversight for research chemicals. Pharmaceutical-grade peptides require a prescription. Self-sourcing is dangerous and not recommended.
How long can I stay on these peptides?
Clinical trials for GLP-1 agonists support long-term use. GH secretagogues are typically cycled (e.g., 8-16 weeks on, 4 weeks off) to prevent desensitization. Continuous use without medical oversight increases risk of adverse effects.
Conclusion: The Future of Fat Loss Is Targeted, But Respect Is Required
The best peptides for fat loss represent a quantum leap in our ability to influence body composition. From the targeted fragment AOD 9604 to the triple receptor agonist Retatrutide, these compounds offer paths for breaking through plateaus that diet and exercise alone could not conquer. Yet their power is directly proportional to the risks when misused. The decision to use any peptide must be anchored in thorough medical consultation, rigorous safety monitoring, and an unshakeable commitment to the fundamentals of nutrition and training. There is no shortcut; there are only smarter, more precise tools.
Whether you choose the appetite-suppressing path of semaglutide, the visceral-shrinking ability of tesamorelin, or the subtle recomposition effects of Ipamorelin, remember that the true goal is not merely a smaller number on the scale, but a healthier, stronger, and more resilient body. Let this guide be your starting point for deeper research, not a substitute for professional advice. The future of fat loss is here—approach it with both ambition and caution.
For more evidence-based fat loss strategies, supplement insights, and performance optimization guides, explore our complete library.
References
- Ng, F. M. et al. "AOD9604, a synthetic analogue of the lipolytic domain of human growth hormone, reduces body weight in obese subjects." International Journal of Obesity, vol. 24, 2000, pp. 118-125.
- Frias, J. P. et al. "Efficacy and safety of co-administered cagrilintide and semaglutide in type 2 diabetes." The Lancet, vol. 398, 2021, pp. 1836-1848.
- Wilding, J. P. H. et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine, vol. 384, 2021, pp. 989-1002.
- Jastreboff, A. M. et al. "Tirzepatide Once Weekly for the Treatment of Obesity." New England Journal of Medicine, vol. 387, 2022, pp. 205-216.
- Rosenstock, J. et al. "Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with obesity: a randomised, double-blind, placebo- and active-controlled, parallel-group, phase 2 trial." The Lancet, vol. 402, 2023, pp. 529-544.
- Falutz, J. et al. "Tesamorelin, a growth hormone-releasing factor, reduces visceral adipose tissue in HIV-infected patients with lipodystrophy." New England Journal of Medicine, vol. 357, 2007, pp. 2359-2370.
- Heffernan, M. A. et al. "The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism in adipocytes." Obesity Research, vol. 9, no. 9, 2001, pp. 553-562.
- Stier, H. et al. "Safety and tolerability of the hexadecapeptide AOD9604 in humans." Journal of Endocrinological Investigation, vol. 36, 2013, pp. 988-994.
- Ng, F. M. & Jiang, W. J. "The lipolytic fragment of human growth hormone: biological activity and mechanism of action." Growth Hormone & IGF Research, vol. 11, 2001, pp. 65-72.
- Teichman, S. L. et al. "Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults." Journal of Clinical Endocrinology & Metabolism, vol. 91, 2006, pp. 799-805.
- Bray, G. A. et al. "The science of obesity management: an Endocrine Society scientific statement." Endocrine Reviews, vol. 39, 2018, pp. 79-132.
- Lean, M. E. J. et al. "Durability of weight loss and metabolic improvements with semaglutide 2.4 mg: 2-year results from STEP 5." Nature Medicine, vol. 29, 2023, pp. 1151-1160.
- Knudsen, L. B. & Lau, J. "The discovery and development of liraglutide and semaglutide." Frontiers in Endocrinology, vol. 10, 2019, p. 155.
- Samms, R. J. et al. "GIPR agonism mediates weight-independent metabolic benefits in obesity." Cell Metabolism, vol. 33, 2021, pp. 1417-1431.
- Müller, T. D. et al. "Glucagon-like peptide 1 (GLP-1)." Molecular Metabolism, vol. 30, 2019, pp. 72-130.
- Christensen, M. et al. "Glucose-dependent insulinotropic polypeptide: from discovery to clinical application." Endocrine Reviews, vol. 32, 2011, pp. 515-548.
- Garber, A. J. et al. "Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm." Endocrine Practice, vol. 25, 2019, pp. 69-100.
- Jarvis, S. et al. "The safety and efficacy of peptide therapies for weight loss: a systematic review." Obesity Reviews, vol. 24, 2023, e13578.
Share