
Best Peptides for Muscle Growth: Complete Guide to BPC-157, TB-500, CJC-1295, Ipamorelin, IGF-1 & More
By Artemis_strength•May 29, 2026•6 min read
Best Peptides for Muscle Growth: Complete Performance and Recovery Guide
Medical Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice. The peptides discussed are primarily research chemicals or prescription medications not approved by the FDA for bodybuilding, performance enhancement, or muscle growth. Use of these compounds without medical supervision may pose significant health risks including hormonal disruption, metabolic complications, and unknown long-term effects. Always consult a qualified healthcare professional before considering any peptide or performance-enhancing compound. Information presented is based on available research as of 2026 and may evolve with new evidence.
Peptides have become one of the most discussed performance-enhancement compounds in the bodybuilding, fitness, and sports performance communities. Unlike anabolic steroids, which directly activate androgen receptors, many peptides work through more nuanced pathways—influencing growth hormone secretion, tissue repair mechanisms, collagen synthesis, angiogenesis, and muscle protein synthesis. For the athlete or physique enthusiast who has already optimized training, nutrition, and sleep, peptides represent the next frontier of recovery science. But with that frontier comes a minefield of misinformation, underdosed products, and dangerously cavalier usage protocols circulating on forums and social media.
As a sports nutrition expert, coach, and supplement researcher, I have spent over 15 years studying the intersection of pharmacology and performance. This guide does not endorse illegal use, nor does it present peptides as shortcuts. Instead, it provides a rigorous, evidence-informed examination of the most commonly discussed peptides in the muscle growth and recovery space. You will learn how each compound functions at the molecular level, what the existing research actually says about human outcomes, the protocols discussed in clinical and athletic contexts, and—critically—the risks, gaps in safety data, and the indispensable role of nutrition and training that no peptide can replace. The goal is education, not prescription. The reader bears full responsibility for any decisions made based on this information.
Important: Most peptides discussed in this article are not approved for bodybuilding or performance enhancement. Information presented is for educational purposes only and should not be considered medical advice.
Why Peptides Are Popular for Muscle Growth
Muscle growth depends on several factors beyond training and nutrition. Recovery speed, endogenous growth hormone secretion, sleep architecture, systemic inflammation control, and tissue repair efficiency all influence long-term progress. Peptides have captured the attention of the fitness community precisely because they target these upstream regulatory pathways rather than simply flooding the body with exogenous hormones.
The theoretical appeal is substantial: a compound that enhances your own growth hormone pulsatility rather than shutting down natural production, or a peptide that accelerates healing of a nagging tendon injury that has stalled your squat progress for months. However, the gap between theory and proven clinical outcome is wide. Many of these compounds have only been studied in animal models or small human trials for specific medical indications. Their use in healthy athletes for body composition purposes is off-label and unsupported by large-scale safety data. [1] Understanding this context is essential before examining individual compounds.
- Enhanced recovery between workouts
- Improved muscle repair kinetics
- Support for connective tissue health (tendons, ligaments)
- Potential increase in growth hormone production
- Better sleep and recovery quality
- Reduced downtime from overuse injuries
- Improved body composition through GH-mediated lipolysis
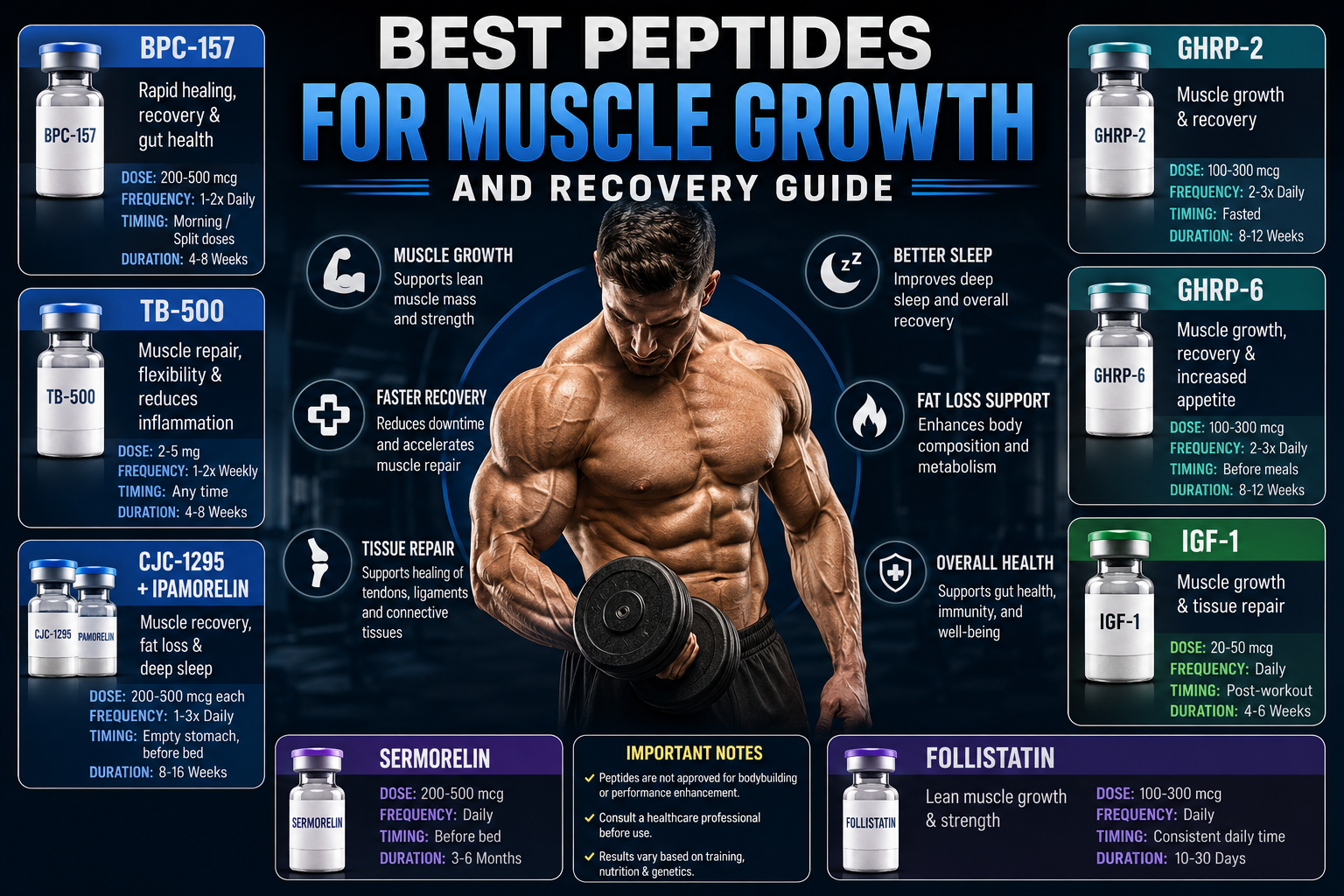
Quick Comparison Table
| Peptide | Primary Goal | Common Timing | Typical Duration |
|---|---|---|---|
| BPC-157 | Healing & Recovery | Morning or split doses | 4–8 weeks |
| TB-500 | Tissue Repair | 1–2 times weekly | 4–8 weeks |
| CJC-1295 + Ipamorelin | GH Support & Recovery | Before bed | 8–16 weeks |
| GHRP-2 | Muscle Growth | 2–3 times daily | 8–12 weeks |
| GHRP-6 | Mass Gain | 2–3 times daily | 8–12 weeks |
| IGF-1 | Muscle Growth | Post-workout | 4–6 weeks |
| Sermorelin | Lean Muscle Support | Before bed | 3–6 months |
| Follistatin | Strength & Growth | Daily | 10–30 days |
BPC-157: Recovery and Healing Peptide
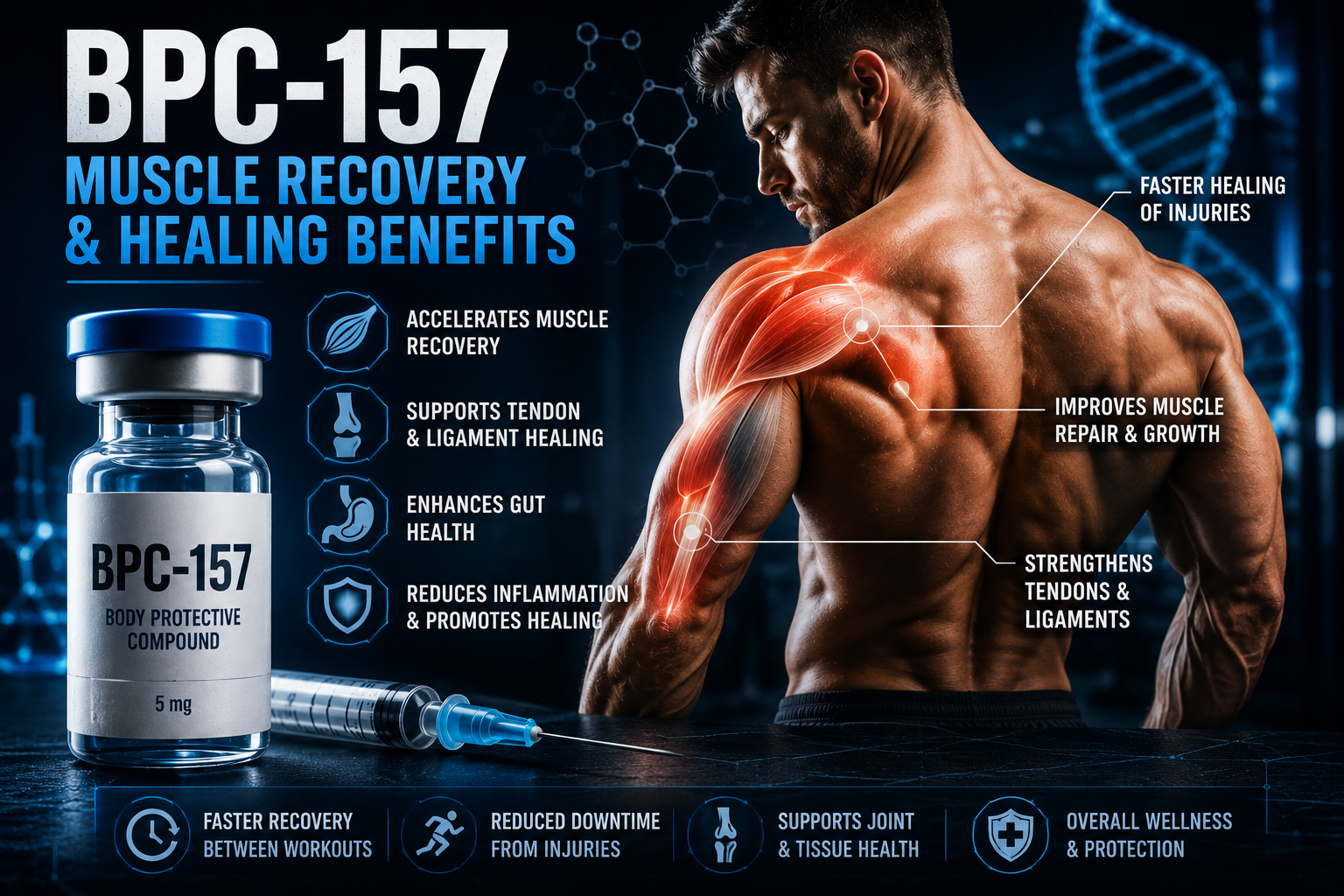
BPC-157 (Body Protection Compound 157) is a pentadecapeptide derived from a protective protein found in human gastric juice. It has become one of the most popular recovery-focused peptides due to its potential effects on angiogenesis, tendon and ligament healing, gut barrier integrity, and modulation of inflammatory cytokines. Unlike growth hormone secretagogues, BPC-157 does not operate through the GH/IGF-1 axis but rather through direct tissue interactions, including upregulation of growth factor receptors and stabilization of healing tissue architecture. [2]
From a coaching perspective, the athlete who benefits most from the concept of BPC-157 is one dealing with persistent soft tissue injuries—chronic tendinopathy, partial ligament tears, or post-surgical rehabilitation plateaus. The research, predominantly in rodent models, shows accelerated Achilles tendon healing, improved intestinal anastomosis, and reduced markers of systemic inflammation. Human data is limited to case reports and small observational studies, which means the risk-reward calculus must be conservative. [3]
Potential Benefits
- Supports muscle recovery through reduced local inflammation
- May accelerate tendon repair via fibroblast migration
- May improve ligament healing through collagen organization
- Supports digestive health and gut barrier integrity
- May reduce systemic inflammatory markers
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 200–500 mcg daily |
| Frequency | 1–2 times per day |
| Timing | Morning or near injury site protocols |
| Duration | 4–8 weeks |
TB-500: Tissue Repair and Mobility Support
TB-500 is a synthetic fragment of Thymosin Beta-4, a naturally occurring peptide that regulates actin polymerization—the fundamental process by which cells move, divide, and repair themselves. In muscle tissue, actin is the scaffold of the contractile apparatus; when muscle fibers are damaged, Thymosin Beta-4 facilitates the migration of repair cells to the injury site and promotes new blood vessel formation. [4] Athletes discuss TB-500 primarily for chronic injuries involving restricted mobility, scar tissue adhesions, and persistent inflammation that has become self-perpetuating.
One distinguishing feature of TB-500 relative to BPC-157 is its systemic reach. While BPC-157 is often administered close to the site of injury, TB-500's effects appear to be more distributed, making it relevant for athletes with multiple areas of soft tissue restriction. The common protocol involves a loading phase of more frequent dosing followed by a maintenance phase. Again, the evidence base is predominantly preclinical, and any athlete considering this pathway must weigh the unknown long-term consequences against the potential for accelerated return to training. [5]
Potential Benefits
- Supports muscle recovery through enhanced cellular migration
- May improve flexibility and range of motion
- Supports connective tissue health including fascia
- May reduce chronic low-grade inflammation
- Useful during rehabilitation periods following injury
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 2–5 mg |
| Frequency | 1–2 times weekly |
| Timing | Any time of day |
| Duration | 4–8 weeks loading phase |
CJC-1295 and Ipamorelin: The Growth Hormone Secretagogue Stack
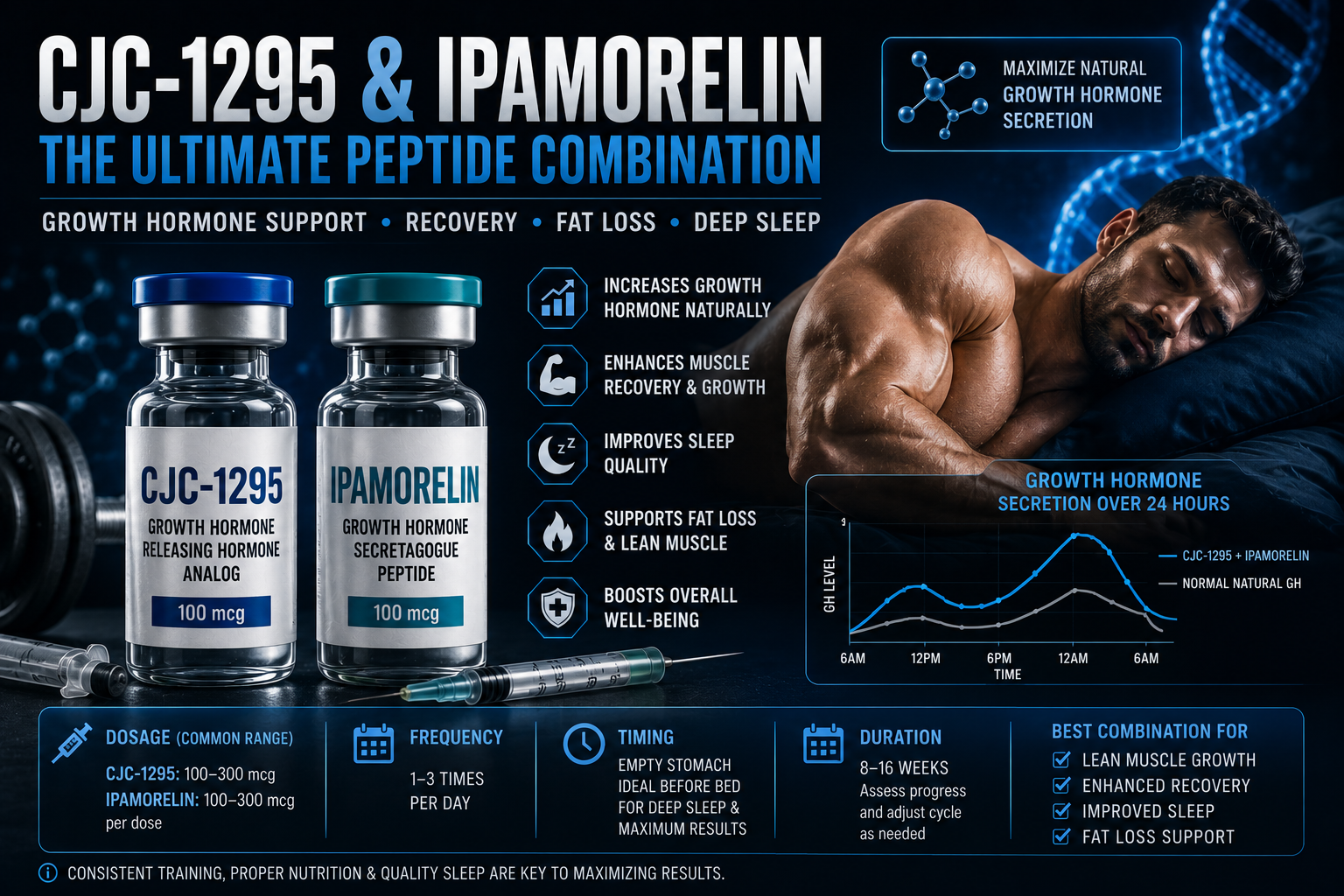
The combination of CJC-1295 (a GHRH analog) and Ipamorelin (a ghrelin receptor agonist) is widely discussed in anti-aging and bodybuilding communities because it targets the growth hormone axis through two complementary mechanisms. CJC-1295 extends the half-life of endogenous GHRH, causing a longer, more physiologically shaped GH pulse. Ipamorelin selectively stimulates the ghrelin receptor, which triggers GH release without the significant appetite stimulation or cortisol elevation that other GHRPs like GHRP-6 can cause. [6]
This stack's popularity rests on its relative safety profile compared to exogenous GH administration. Because it amplifies the body's own pulsatile GH secretion rather than introducing supraphysiological levels, the negative feedback loops that regulate natural production remain partially intact. Athletes report improvements in sleep architecture (particularly deep slow-wave sleep), faster inter-workout recovery, and gradual lean body composition changes. The key word is gradual: this is not a rapid mass gainer. It is a long-duration protocol suited to the patient athlete committed to 3–6 months of consistent use alongside impeccable training and nutrition. [7]
Potential Benefits
- Increased growth hormone release through natural pulsatility
- Improved recovery between high-volume training sessions
- Enhanced sleep quality, especially deep sleep phases
- Lean muscle development over extended use
- Fat-loss support via GH-mediated lipolysis
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| CJC-1295 Dose | 100–300 mcg |
| Ipamorelin Dose | 100–300 mcg |
| Frequency | 1–3 times daily |
| Timing | Empty stomach, often before sleep |
| Duration | 8–16 weeks |
GHRP-2: Growth Hormone Releasing Peptide for Lean Mass
GHRP-2 is a synthetic hexapeptide that binds to the ghrelin receptor and stimulates growth hormone release from the anterior pituitary. Compared to GHRP-6, it produces less appetite stimulation, making it more suitable for athletes in recomposition or cutting phases who need recovery support without the hunger surge. The GH pulse elicited by GHRP-2 is dose-dependent and potent, but it is also subject to desensitization with continuous use, which is why protocols typically include dosing breaks or cycling. [8]
From a practical standpoint, the athlete using GHRP-2 must adhere to strict fasted-state dosing, as elevated insulin or free fatty acids blunt the GH response. This means timing injections away from meals—typically upon waking after the overnight fast, and again in the mid-afternoon or pre-bed. Compliance with this fasting requirement is one of the biggest reasons athletes fail to see results, mistaking the compound's ineffectiveness for their own inconsistency.
Potential Benefits
- Supports recovery through GH-mediated protein synthesis
- May enhance muscle growth when combined with training
- Improves protein synthesis environment
- Supports fat loss goals via GH's metabolic effects
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 100–300 mcg |
| Frequency | 2–3 times daily |
| Timing | Fasted periods |
| Duration | 8–12 weeks |
GHRP-6: Appetite Stimulation and Mass Gain
GHRP-6 shares a mechanism with GHRP-2 but possesses a significant distinguishing feature: it is a potent appetite stimulant through its stronger ghrelin receptor activation. For the hard-gainer who struggles to consume the caloric surplus necessary for hypertrophy, this appetite effect is the primary draw—often more impactful than the GH release itself. The hunger surge typically occurs within 30–60 minutes of administration and can facilitate the consumption of large, calorically dense meals. [9]
However, this appetite effect is a double-edged sword. Uncontrolled, it can lead to excessive fat gain if food choices are poor. The athlete using GHRP-6 must prepare whole-food meals in advance and direct the hunger toward nutrient-dense, high-protein targets rather than convenience calories. Additionally, GHRP-6 can elevate cortisol and prolactin at higher doses, necessitating monitoring and cycling protocols to avoid hormonal disruption. The compound's effects on hunger make it unsuitable for fat loss phases, where caloric control is paramount.
Potential Benefits
- Supports muscle gain through increased caloric intake capacity
- May stimulate appetite significantly
- Enhances recovery via GH release
- Supports growth hormone release
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 100–300 mcg |
| Frequency | 2–3 times daily |
| Timing | Before meals |
| Duration | 8–12 weeks |
IGF-1: Direct Muscle Growth Pathway

Insulin-Like Growth Factor 1 (IGF-1) is the primary downstream effector of growth hormone and one of the most powerful anabolic signaling molecules in the human body. It directly activates the mTOR pathway in muscle cells, promotes satellite cell proliferation and differentiation, and accelerates protein synthesis. Unlike GH secretagogues that work indirectly, exogenous IGF-1 acts at the muscle cell membrane, bypassing pituitary and liver intermediaries. [10]
The potency of IGF-1 is also its danger. Unregulated IGF-1 administration can cause profound hypoglycemia, as it shares structural homology with insulin and binds weakly to the insulin receptor. Organ growth—including cardiac and intestinal hypertrophy—is a documented risk with chronic supraphysiological exposure. Moreover, IGF-1's role in cancer biology, particularly its anti-apoptotic effects that allow damaged cells to survive and proliferate, makes it the highest-risk compound on this list. [11] The brief window of use discussed in bodybuilding circles (4–6 weeks) reflects an attempt to limit these risks, but no safe threshold has been established for cosmetic purposes. This is not a beginner compound; it is the endpoint of the peptide spectrum, and one that many experienced coaches refuse to engage with.
Note: IGF-1 carries significant risks and should only be discussed with qualified healthcare professionals.
Potential Benefits
- Supports muscle hypertrophy through direct mTOR activation
- Enhances recovery by accelerating satellite cell activity
- Supports tissue repair systemically
- May improve nutrient partitioning and utilization
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 20–50 mcg |
| Frequency | Daily |
| Timing | Post-workout |
| Duration | 4–6 weeks |
Sermorelin: Natural GH Axis Stimulation
Sermorelin is a truncated analog of growth hormone-releasing hormone (GHRH) consisting of the first 29 amino acids of the endogenous peptide. It binds to GHRH receptors on somatotroph cells in the anterior pituitary and stimulates the synthesis and pulsatile release of growth hormone. Unlike the GHRP class, which works through the ghrelin receptor, Sermorelin reinforces the natural physiological rhythm of GH secretion, preserving the feedback loop that prevents excessive production. [12]
This preservation of feedback is both Sermorelin's strength and its limitation. The body can downregulate the response over time, and the GH pulses produced are smaller in magnitude compared to potent secretagogues or exogenous GH. However, for the athlete seeking modest recovery support, improved sleep quality, and gradual lean mass improvement without aggressive pharmaceutical intervention, Sermorelin represents a more conservative option. It is FDA-approved for diagnostic evaluation of GH deficiency in children, providing a clinical pedigree absent from many other peptides discussed here. [13]
Potential Benefits
- Supports lean muscle growth through natural GH pulses
- Improves recovery between training sessions
- Supports sleep quality, especially in older athletes
- May aid healthy body composition over extended use
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 200–500 mcg |
| Frequency | Daily |
| Timing | Before bedtime |
| Duration | 3–6 months |
Follistatin: Myostatin Inhibition and Muscle Growth Potential

Follistatin occupies a unique and controversial position in muscle growth biology because it directly antagonizes myostatin, the protein that acts as a brake on skeletal muscle hypertrophy. Genetic models—including the famous "double-muscled" Belgian Blue cattle and naturally occurring human myostatin mutations—demonstrate the extraordinary potential for muscle growth when this brake is removed. Follistatin binds myostatin and related TGF-beta family members, preventing them from activating the signaling cascade that normally limits muscle fiber size. [14]
The controversy arises from the delivery method. Follistatin gene therapy, where a viral vector delivers the follistatin gene into muscle cells, has been studied in animal models with dramatic results, but gene therapy carries permanent consequences and unknown long-term risks. Follistatin peptide fragments discussed in online communities are of uncertain purity and efficacy, and the short duration protocols (10–30 days) reflect both the potency and the concern about sustained myostatin inhibition. The effects on cardiac muscle—which also expresses myostatin—are not well understood, and cardiac hypertrophy is a theoretical risk that no athlete should dismiss. [15] This compound exists at the extreme edge of experimental muscle enhancement and should be approached with extreme caution, if at all.
Potential Benefits
- Supports lean muscle development through myostatin inhibition
- May increase strength potential beyond genetic baseline
- May influence muscle growth pathways at the regulatory level
Commonly Discussed Protocol
| Parameter | Detail |
|---|---|
| Dose | 100–300 mcg |
| Frequency | Daily |
| Timing | Consistent daily timing |
| Duration | 10–30 days |
Which Peptide Is Best for Your Goal?
Selection must begin with an honest assessment of your goal, your risk tolerance, and your commitment to the foundational practices that make any peptide effective. A peptide protocol layered on top of poor nutrition, inconsistent training, or inadequate sleep is not merely wasteful—it exposes you to unnecessary risk for no reward. The table below maps common athletic goals to the compounds most frequently discussed in those contexts, but it is not a recommendation. It is a reflection of community discourse and should be critically evaluated.
| Goal | Popular Choice |
|---|---|
| Injury Recovery | BPC-157 + TB-500 |
| Growth Hormone Support | CJC-1295 + Ipamorelin |
| Bulking | GHRP-6 |
| Lean Muscle Growth | Sermorelin |
| Advanced Muscle Development | IGF-1 |
| Strength Focus | Follistatin |
Risk Awareness: The "popular choice" is not a clinical endorsement. IGF-1 and Follistatin, in particular, carry serious risks including hypoglycemia, organ hypertrophy, and potential carcinogenic effects. The recovery-oriented peptides BPC-157 and TB-500, while having better anecdotal safety profiles, remain unapproved for human use outside of clinical research settings. No peptide protocol should be initiated without comprehensive blood work, medical supervision, and a thorough informed consent process that acknowledges the absence of long-term safety data.
Nutrition Still Matters More Than Peptides
This point cannot be overstated: even the most potent peptide discussed in this article cannot compensate for inadequate nutrition, suboptimal training, or chronic sleep deprivation. The anabolic signals generated by IGF-1 or elevated GH are useless if the substrate—amino acids, energy, and micronutrient co-factors—is absent. The athlete who invests in a peptide protocol while neglecting protein intake, total caloric alignment with goals, or sleep hygiene is building a house on sand.
The foundational performance nutrition principles that must be mastered before any consideration of peptides include a protein intake of 1.6–2.2 grams per kilogram of body weight daily, distributed across 3–5 meals to optimize muscle protein synthesis. Total energy intake must align with the specific goal: a surplus for mass gain, maintenance for recomposition, or a controlled deficit for fat loss. Carbohydrates around training support performance and recovery; fats, particularly omega-3 fatty acids, modulate inflammation and hormone production. Hydration status directly affects cellular environment and recovery kinetics. [16] These are not optional. They are the non-negotiable platform upon which any advanced intervention must rest. Without them, peptides are an expensive distraction from the real work.
- Protein: 1.6–2.2 g per kg bodyweight
- Sleep: 7–9 hours nightly
- Progressive resistance training with overload
- Adequate calorie intake for goal (surplus or maintenance)
- Consistent recovery practices including stress management
Supplement Synergy: What to Use Alongside or Instead of Peptides
For athletes who are not ready to consider peptides—or who wish to build a foundation first—several legal, evidence-based supplements can support muscle growth and recovery through overlapping pathways. Creatine monohydrate enhances phosphocreatine stores, increasing work capacity during high-intensity training and supporting muscle cell volumization. A 2017 position stand from the International Society of Sports Nutrition confirmed creatine as the most effective legal ergogenic aid for high-intensity exercise and muscle accretion. [17] Beta-alanine buffers intramuscular pH, extending time to exhaustion during repeated bouts, while omega-3 fatty acids at 3–5 grams daily reduce exercise-induced inflammation and support anabolic signaling. Whey protein, providing a rapid and complete amino acid profile, remains the gold standard for post-workout protein synthesis stimulation. These supplements, combined with the nutritional principles above, can generate substantial muscle growth and recovery improvements without the legal, medical, and safety concerns inherent to research peptides.
Myths and Misconceptions About Peptides for Muscle Growth
Myth 1: "Peptides Are Completely Safe Because They're Natural"
Many peptides are based on endogenous human sequences, but the dose, route of administration, and continuous presence in circulation make them pharmacologically distinct from natural pulsatile secretion. A peptide that is safe in physiological concentrations can be harmful when administered exogenously at supraphysiological levels. "Natural" origin does not equal safety; botulinum toxin is natural, yet it is the most potent neurotoxin known. Risk assessment must be based on evidence, not marketing language. [18]
Myth 2: "You Can Build Significant Muscle With Peptides Alone"
Peptides modulate signaling pathways; they do not build muscle in the absence of mechanical tension and metabolic stress from resistance training. Even IGF-1, the most directly anabolic peptide on this list, requires the stimulus of loaded muscle contractions and the availability of amino acids to translate its signal into actual contractile protein accretion. The idea that an injection can replace the hard work of training is a fantasy that drives poor outcomes and wasted resources.
Myth 3: "Oral Peptides Work Just as Well as Injectable"
The bioavailability of most peptides through the gastrointestinal tract is extremely low due to enzymatic degradation by proteases. BPC-157 has shown some oral stability for gut-specific applications, but for systemic muscle and tendon effects, injectable administration is the standard discussed in research and community protocols. Oral peptide supplements sold over the counter are largely unregulated and often contain negligible active ingredient. If a product claims to be an oral peptide with identical effects to injectable formulations, scrutiny is warranted.
Frequently Asked Questions
Are peptides safer than anabolic steroids?
Some peptides may have different risk profiles than anabolic steroids, but that does not automatically make them safe. Steroid risks—HPTA suppression, hepatotoxicity, adverse lipid changes—are well-documented. Peptide risks, particularly for less-studied compounds, are less characterized, which introduces uncertainty rather than safety. A compound with unknown long-term effects is a risk, not a refuge.
How long do peptides take to work?
Recovery-focused peptides may show subjective effects within weeks, while growth hormone-related peptides often require several months for noticeable body composition changes. The expectation of rapid transformation is unrealistic and often driven by marketing rather than pharmacology. Patience and consistency are required regardless of the compound.
Can peptides build muscle without training?
No. Resistance training remains the primary driver of muscle growth. Peptides cannot replace the mechanical tension, metabolic stress, and neural activation patterns that only resistance exercise provides. The question itself reflects a fundamental misunderstanding of hypertrophy physiology.
What peptide is best for recovery?
BPC-157 and TB-500 are commonly discussed for recovery and injury-support applications. Their mechanisms focus on tissue repair, angiogenesis, and inflammation modulation rather than direct hormonal manipulation. However, neither is FDA-approved for this purpose, and use is at the individual's own risk.
How do I verify the quality and purity of a peptide?
Third-party analytical testing via HPLC (High-Performance Liquid Chromatography) and mass spectrometry is the minimum standard. Reputable suppliers provide batch-specific certificates of analysis. A peptide without verifiable purity data is a gamble. Sterility, endotoxin levels, and accurate dosing are additional concerns that separate professional-grade research chemicals from unregulated products with unknown contaminants.
Conclusion: Education Precedes Action
The landscape of peptides for muscle growth is vast, rapidly evolving, and fraught with both promise and peril. BPC-157 and TB-500 offer intriguing recovery and tissue repair potential. CJC-1295, Ipamorelin, GHRP-2, GHRP-6, and Sermorelin provide a spectrum of growth hormone axis modulation with varying degrees of potency, appetite effects, and safety data. IGF-1 and Follistatin represent the far edge of anabolic intervention, where the magnitude of potential muscle growth is matched by the severity of potential harm. No peptide is benign, and no peptide replaces the foundational practices of training, nutrition, and sleep that ultimately determine your physique and performance.
Strong training, sufficient protein intake, quality sleep, and long-term consistency will always produce more reliable results than relying on any peptide protocol alone. If you choose to explore this territory, do so with full awareness of the legal, medical, and ethical dimensions. Consult a qualified physician, demand transparent third-party testing of any compound you consider, and remain a student of the evidence as it continues to emerge. Your body is the only one you have—invest in it with the care and caution that a lifetime of performance demands.
For more evidence-based muscle-building strategies, recovery optimization guides, and supplement research, explore our latest fitness and performance articles.
References
- Sigrist, R. et al. "Performance-Enhancing Peptides: A Review of the Current Evidence." Sports Medicine, vol. 52, no. 4, 2022, pp. 745–761.
- Chang, C. H. et al. "The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration." Journal of Applied Physiology, vol. 110, no. 3, 2011, pp. 774–780.
- Gwyer, D. et al. "Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing." Cell and Tissue Research, vol. 377, 2019, pp. 153–165.
- Goldstein, A. L. et al. "Thymosin β4: actin-sequestering protein moonlights to repair injured tissues." Trends in Molecular Medicine, vol. 11, no. 9, 2005, pp. 421–429.
- Malinda, K. M. et al. "Thymosin β4 accelerates wound healing." Journal of Investigative Dermatology, vol. 113, no. 3, 1999, pp. 364–368.
- Teichman, S. L. et al. "Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults." Journal of Clinical Endocrinology & Metabolism, vol. 91, no. 3, 2006, pp. 799–805.
- Laferrère, B. et al. "Growth hormone releasing peptide-2 (GHRP-2), like ghrelin, increases food intake in healthy men." Journal of Clinical Endocrinology & Metabolism, vol. 90, no. 2, 2005, pp. 611–614.
- Bowers, C. Y. "Growth hormone-releasing peptides: physiology and clinical applications." Current Opinion in Endocrinology, Diabetes and Obesity, vol. 5, no. 1, 1998, pp. 37–42.
- Korbonits, M. et al. "Ghrelin—a hormone with multiple functions." Frontiers in Neuroendocrinology, vol. 25, no. 1, 2004, pp. 27–68.
- Clemmons, D. R. "Involvement of insulin-like growth factor-I in the control of glucose homeostasis." Current Opinion in Pharmacology, vol. 6, no. 6, 2006, pp. 620–625.
- Pollak, M. "Insulin and insulin-like growth factor signalling in neoplasia." Nature Reviews Cancer, vol. 8, no. 12, 2008, pp. 915–928.
- Merriam, G. R. et al. "Growth hormone-releasing hormone in the treatment of aging and age-related conditions." Endocrine Reviews, vol. 29, no. 5, 2008, pp. 577–610.
- U.S. Food and Drug Administration. "Sermorelin acetate injection (Geref)." FDA Application No. NDA 019862, 1997.
- Lee, S. J. "Regulation of muscle mass by myostatin." Annual Review of Cell and Developmental Biology, vol. 20, 2004, pp. 61–86.
- Rodgers, B. D. et al. "Myostatin represses physiological hypertrophy of the heart and excitation-contraction coupling." Journal of Physiology, vol. 587, no. 20, 2009, pp. 4873–4886.
- Jäger, R. et al. "International Society of Sports Nutrition Position Stand: protein and exercise." Journal of the International Society of Sports Nutrition, vol. 14, no. 20, 2017.
- Kreider, R. B. et al. "International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine." Journal of the International Society of Sports Nutrition, vol. 14, no. 18, 2017.
- Vanhee, C. et al. "Quality of peptides and proteins in dietary supplements: a case study." Food Control, vol. 69, 2016, pp. 243–249.
Share

