Breast Milk vs Formula: The Biological Truth Every Parent Must Understand for Lifelong Infant Health
By Artemis_strength•12 min read
Breast Milk vs Formula: The Biological Truth Every Parent Must Understand for Lifelong Infant Health
Few decisions in early parenthood carry more biological weight than how to feed a newborn. The breast milk versus formula debate is not a matter of lifestyle preference—it is a conversation rooted in cellular biology, immunology, and developmental programming. At our editorial desk of sports nutritionists, lactation scientists, and pediatric researchers, we refuse to frame this as a moral argument. Instead, we present the unvarnished scientific data, showing exactly what happens inside an infant’s body when it receives human milk versus manufactured substitutes. Understanding these differences empowers parents to make informed decisions and, whenever possible, to leverage the unique properties of breast milk to shape a child’s lifelong health trajectory.
Key Takeaway: Breast milk is a dynamic, living tissue containing stem cells, immune cells, enzymes, hormones, and a personalized microbiome that changes hourly in response to the infant. Formula, while nutritionally complete for survival and growth, is a static, dead product that cannot replicate the bioactive dialogue between mother and child. The health gap is not about macronutrients—it is about the orchestration of gene expression, gut maturation, and immune tolerance that only breastfeeding provides.
What Makes Breast Milk a Living Substance: Beyond Simple Nutrition
Human milk is not a uniform fluid. It is a biological system that varies by time of day, duration of feeding, infant age, and even the baby’s infection status. A 2023 single-cell RNA sequencing study identified over 25 distinct cell types in human milk, including multipotent stem cells capable of differentiating into bone, cartilage, and neural tissue. These cells survive digestion and may engraft into the infant’s organs, contributing to tissue repair and long-term cellular function. No formula on earth contains a single living cell. This distinction alone fundamentally shifts the conversation from “both provide calories” to “only one delivers biological instructions.”
Macronutrient Landscape: Similar Numbers, Radically Different Structures
At first glance, standard infant formula appears to match breast milk’s protein, fat, and carbohydrate content. But this numeric equivalence conceals molecular chasms.
| Component | Human Breast Milk | Standard Infant Formula |
|---|---|---|
| Protein | 60:40 whey-to-casein ratio, rich in alpha-lactalbumin and lactoferrin; easily digested, non-allergenic human proteins; contains immunoglobulins | Variable whey:casein, often bovine beta-lactoglobulin (common allergen); proteins are heat-denatured during processing; no antibodies |
| Fats | Cholesterol (essential for myelin), long-chain polyunsaturated fatty acids DHA/ARA in natural phospholipid form, milk fat globule membrane (MFGM) aiding neural development, lipase enzyme for self-digestion | Vegetable oil blends, added synthetic DHA/ARA (algal/fungal) without natural MFGM; lacks cholesterol; no lipase |
| Carbohydrates | Lactose primary; over 200 structurally distinct human milk oligosaccharides (HMOs) that feed beneficial Bifidobacteria and block pathogen binding | Lactose; some formulas add one or two HMO mimics (2'-FL, LNnT) but cannot replicate the diversity; often rely on simpler prebiotics like GOS/FOS |
| Bioactive Matrix | Contains live cells, mRNA, microRNA, cytokines, growth factors (EGF, IGF-1, TGF-β), enzymes, hormones (leptin, adiponectin), and maternal antibodies | None; pasteurized, sterilized, and powdered; no signaling molecules survive industrial processing |
The fat fraction deserves special attention. Breast milk delivers cholesterol at concentrations triple that of formula—an absolute requirement for constructing the myelin sheaths that insulate neurons and enable rapid signal transmission. The milk fat globule membrane (MFGM) surrounding breast milk lipid droplets is rich in phospholipids and gangliosides that independently improve cognitive outcomes in formula-fed infants when added, yet only human milk provides them in their natural, perfectly integrated configuration. The enzyme bile salt-stimulated lipase, unique to human milk, actively digests fats in the newborn’s immature gut, effectively compensating for the infant’s own low pancreatic enzyme output.
The Immune Command Center: How Breast Milk Replaces the Immature Immune System
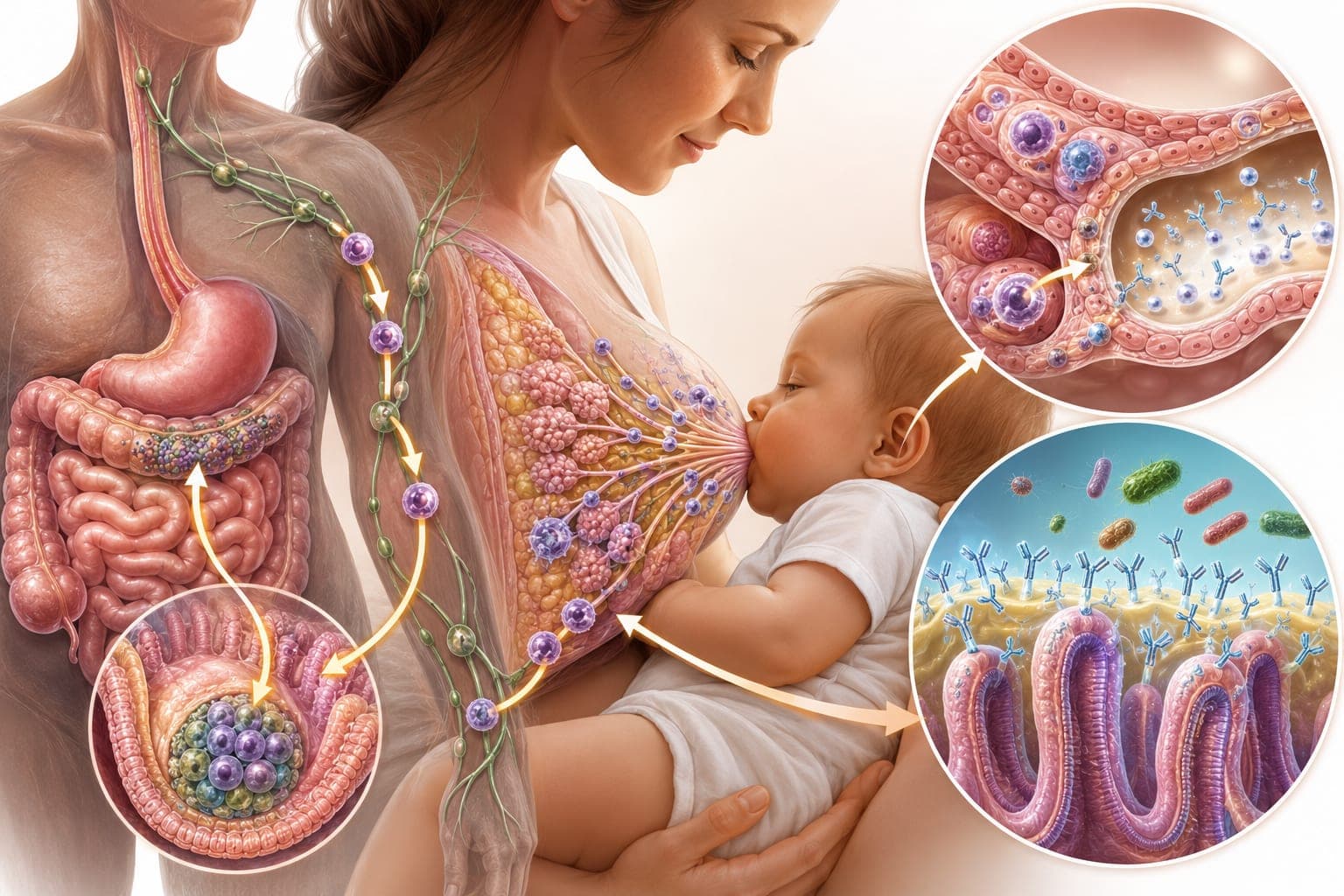
A newborn enters the world with a deliberately naive immune system—if fully matured in utero, it would reject maternal tissue. Breast milk acts as a temporary transplant of the mother’s immunological competence. The entero-mammary axis is the critical mechanism: when a mother’s gut encounters a pathogen, specialized plasma cells traffic to her mammary glands and secrete pathogen-specific secretory IgA into her milk within hours. The infant swallows these antibodies, which then coat the nasopharynx and gut epithelium, neutralizing viruses and bacteria before they invade. This real-time immune surveillance cannot be replicated in a factory.
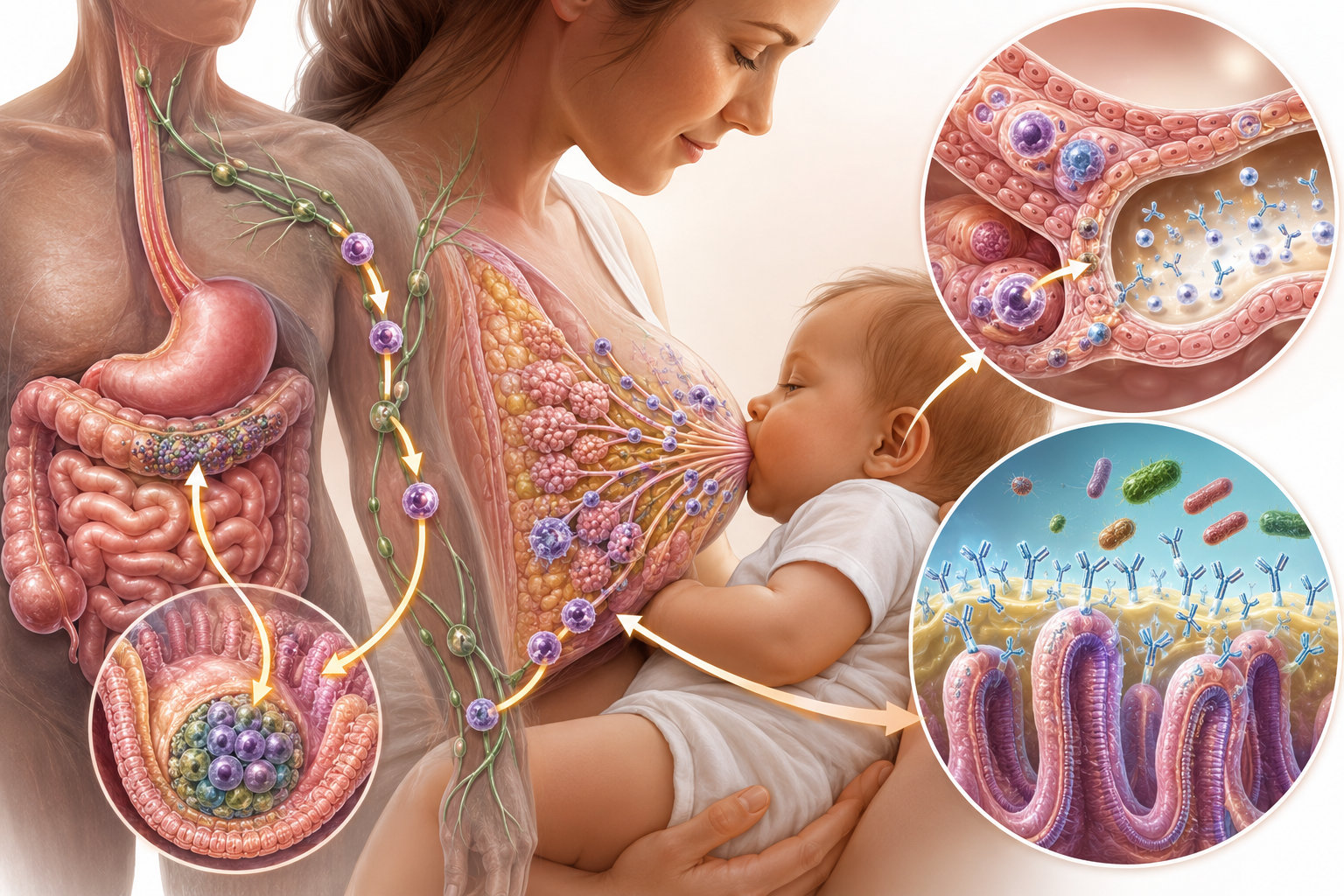
Beyond antibodies, breast milk delivers lactoferrin—an iron-binding protein that starves pathogenic bacteria while promoting beneficial Lactobacillus growth—and lysozyme, which directly lyses bacterial cell walls. Human milk oligosaccharides (HMOs) function as decoy receptors: they structurally mimic the gut epithelial cell surface carbohydrates to which pathogens bind, so bacteria and viruses attach to the soluble HMOs instead and are harmlessly flushed out. A 2016 multicenter study in Pediatrics calculated that exclusive breastfeeding for six months reduces infant hospitalization for lower respiratory tract infections by 72% and gastrointestinal infections by 64% compared to formula feeding. This is not about hygiene; it is about biological weaponry that formula cannot supply.
Long-Term Health Outcomes: Metabolic and Neurodevelopmental Programming
The Developmental Origins of Health and Disease (DOHaD) framework has established that early nutrition permanently programs an individual’s risk for obesity, diabetes, cardiovascular disease, and neurocognitive deficits. Breastfeeding exerts a dose-response protective effect. A pooled analysis of 17 studies found that each month of exclusive breastfeeding is associated with a 4% reduction in later obesity risk. The mechanisms are multifactorial: breast milk contains leptin and adiponectin, hormones that regulate appetite and insulin sensitivity, which cross the intestinal barrier and tune the infant’s hypothalamic feeding circuits. Formula, devoid of these hormones, may permit an upward resetting of the body’s adiposity set-point.
On the neurological front, the data consistently show a 2–3 point increase in childhood IQ among breastfed cohorts after adjusting for maternal education and socioeconomic status. The largest effect is seen in preterm infants, where breast milk intake correlates with significantly larger total brain volume and white matter integrity at term-equivalent age on MRI. The responsible agents include DHA, cholesterol, choline, sialic acid, and the hormonal milieu that fosters synapse formation and myelination. One underappreciated finding: the act of breastfeeding itself—with its rhythmic suckling, skin-to-skin contact, and oxytocin release in both mother and infant—induces a parasympathetic state that facilitates deeper sleep and memory consolidation, an effect absent from bottle-feeding of expressed milk or formula.
Modern Formula Advancements: Bridging the Gap, Not Closing It
Formula manufacturers have made genuine strides. The addition of two HMOs (2'-fucosyllactose and lacto-N-neotetraose) to some formulas has shifted stool microbiota closer to that of breastfed infants and modestly reduced parental reports of respiratory illness. MFGM-supplemented formulas have demonstrated a 2–3 point cognitive advantage over standard formula at 12 months in randomized trials. Yet these additions remain isolated, industrial approximations. The synergistic complexity of over 200 HMOs interacting with live maternal cells, cytokines, and microRNAs cannot be bottled. Parents who use formula should select products containing DHA/ARA at 0.32% and 0.64% of total fat respectively, plus MFGM and HMOs, to partially narrow the health gap, but they must understand that even the most advanced formula remains a supplement to—not a replacement for—the living matrix.
Pro Tip for Formula-Feeding Parents: Practice “responsive bottle-feeding” with paced bottle feeding techniques: hold the baby semi-upright, use a slow-flow nipple, pause every 20-30 seconds, and switch sides mid-feed. This mimics breastfeeding’s autonomic regulation, reduces overfeeding risk, and preserves the infant’s innate appetite control.
Practical Considerations: Safety, Cost, and Maternal Health
Critics of exclusive breastfeeding advocacy often cite the physical and economic realities. Formula costs range from $1,200 to $3,000 annually per infant, while breastfeeding requires substantial maternal time (approximately 1,800 hours in the first year—equivalent to a full-time job) and carries its own burdens: cracked nipples, mastitis, and the mental load of being the sole nutritional source. However, framing this as a simple consumer choice obscures the larger economic calculus. A 2019 cohort study in The Lancet estimated that suboptimal breastfeeding rates cost the global economy $302 billion annually in lost human capital and healthcare expenditures. For the individual mother, breastfeeding reduces her lifetime risk of breast cancer (4.3% reduction for every 12 months of lactation) and ovarian cancer, mediated by suppressed ovulation and differentiation of breast ductal tissue. Formula feeding confers no reciprocal protection. These data matter for fully informed consent.
Common Myths vs. Facts
- Myth: “Modern formula is almost identical to breast milk.”
Fact: Formula matches gross macronutrient percentages but contains no living cells, no maternal antibodies, no dynamic HMO diversity, no responsive enzyme activity. Calling it “almost identical” is akin to saying a textbook photo of the ocean is almost identical to standing on the shore—informationally shallow and functionally inert. - Myth: “Breastfeeding past 12 months offers no nutritional benefit.”
Fact: Human milk continues to provide significant calories, protein, vitamins, and immune factors well beyond one year. The World Health Organization recommends continued breastfeeding up to two years and beyond as part of a complementary diet, and anthropological evidence suggests natural weaning ages between 2.5 and 7 years. - Myth: “Formula-fed babies sleep better because formula is heavier.”
Fact: Formula empties from the stomach more slowly due to its higher casein content, creating a sensation of prolonged fullness, but this does not equate to healthier sleep architecture. Breastfed infants rouse more frequently, which may actually be protective against SIDS by preventing excessively deep sleep periods in the first months. - Myth: “If I need to supplement with formula, I might as well stop breastfeeding.”
Fact: The benefit of breast milk is dose-dependent. Any amount of breast milk confers immune and developmental advantages that increase with exclusivity. Partial breastfeeding retains significant value; mothers should be supported in mixed feeding without being told it is “all or nothing.”
Frequently Asked Questions
Is it true that breast milk can cure infections in the baby?
Breast milk is not a pharmaceutical cure, but it is a dynamic immune therapeutic. During an infection, the mother’s body receives immunological signals through the infant’s saliva during suckling, potentially via retrograde flow into the mammary ducts. This triggers a rapid increase in leukocyte concentration and pathogen-specific antibodies in the next feed. Milk applied topically to minor cuts, conjunctivitis, or diaper rash has antibacterial and anti-inflammatory effects, though severe infections require medical treatment.
Can I make my own formula at home to avoid commercial products?
No. Homemade infant formulas are dangerously inadequate and have been associated with severe electrolyte imbalances, infection, and infant death. The precise nutrient balance required for infant survival—mineral ratios, iron, vitamin D, essential fatty acids—cannot be replicated in a home kitchen. If formula is necessary, only commercially prepared products meeting FDA or equivalent regulatory standards should be used.
What happens in the baby’s gut when switching from breast milk to formula?
Within 24 hours of the first formula feed, the infant gut microbiome shifts dramatically. The protective Bifidobacterium-dominant flora, nourished by HMOs, declines rapidly, replaced by a more adult-like and potentially more pathogenic mix of Enterobacteriaceae, Bacteroides, and Clostridia. This microbial shift is accompanied by increased gut permeability and a measurable rise in inflammatory markers. Exclusive breastfeeding maintains a gut environment optimized for immune tolerance and pathogen resistance.
How long does it take for breast milk to provide antibodies after the mother gets sick?
The entero-mammary immune response begins within hours of maternal pathogen exposure. By the next feed, specific IgA antibodies can be detected in her milk, peaking around 24–48 hours. This is why continuing to breastfeed through a minor maternal illness is not only safe but actively protective for the infant.
Does breast milk from a mother who eats poorly have less nutritional value than formula?
Remarkably, breast milk maintains adequate macronutrient content even on a suboptimal maternal diet because the mammary gland preferentially draws from maternal stores. The price is paid by the mother in terms of depleted nutrient reserves. However, the micronutrient quality—vitamin B12, iodine, DHA, and vitamin D—can suffer if maternal intake is chronically low. A well-supplemented mother produces milk with superior fatty acid and vitamin profiles. Even “poor-quality” breast milk still contains live immune cells and HMOs absent from formula.
Conclusion: Informed Choices Empower Better Outcomes
The breast milk vs formula debate, stripped of guilt and judgment, resolves into a clear biological reality: human milk is a living, personalized medicine that no industrial process can duplicate. This is not a moral statement; it is a scientific one. Every drop of breast milk delivers stem cells, antibodies, and hormonal signals that program the infant for a lifetime of resilience. Formula is a life-saving, safe alternative when breastfeeding is impossible or insufficient, and modern enhancements are narrowing some outcome gaps, but the irreducible difference remains. We urge every expectant parent to seek prenatal lactation education, to establish a supportive feeding plan with an IBCLC, and to understand that partial breastfeeding still matters immensely. For those navigating exclusive formula feeding, choose a product with DHA, MFGM, and HMOs, practice paced feeding, and know that love, not just milk, builds a brain. Download our free “Infant Feeding Decision Tool” to evaluate your unique circumstances with our team of prenatal nutrition coaches—because an informed choice is always the best choice.
Medical & Health Disclaimer
The content in this article is for educational and informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your pediatrician, family physician, or a board-certified lactation consultant regarding any infant feeding decisions. Never delay or disregard medical guidance based on information read here.
Scientific References
- Victora CG, Bahl R, Barros AJD, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475-490.
- Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. 2013;60(1):49-74.
- Hassiotou F, Hartmann PE. At the dawn of a new discovery: the potential of breast milk stem cells. Adv Nutr. 2014;5(6):770-778.
- Martin CR, Ling PR, Blackburn GL. Review of infant feeding: key features of breast milk and infant formula. Nutrients. 2016;8(5):279.
- Andreas NJ, Kampmann B, Mehring Le-Doare K. Human breast milk: a review on its composition and bioactivity. Early Hum Dev. 2015;91(11):629-635.
- Bode L. Human milk oligosaccharides: every baby needs a sugar mama. Glycobiology. 2012;22(9):1147-1162.
- Deoni SCL, Dean DC III, Piryatinsky I, et al. Breastfeeding and early white matter development: a cross-sectional study. Neuroimage. 2013;82:77-86.
- Rollins NC, Bhandari N, Hajeebhoy N, et al. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016;387(10017):491-504.
Share