How a Mother’s Diet Shapes Breast Milk: The Science of Nutrient Transfer for Optimal Infant Development
By Artemis_strength•June 9, 2026•11 min read
How a Mother’s Diet Shapes Breast Milk: The Science of Nutrient Transfer for Optimal Infant Development
Breast milk is often described as the perfect food—dynamic, responsive, and uniquely tailored to an infant’s needs. But it is not a static, magical fluid. Lactation biology reveals that breast milk composition continually adapts based on maternal nutritional status, dietary intake, hydration, and even environmental signals. For the fitness-conscious, health-savvy mother, understanding exactly which foods affect breast milk and how they act as a biological bridge to the infant’s developing brain, immune system, and gut microbiome is essential. Here, our team of certified sports nutritionists, lactation researchers, and fitness coaches dissects the precise mechanisms by which maternal diet shapes breast milk, dispels pervasive myths, and provides an evidence-based nutritional blueprint for nursing mothers who demand the very best for their child’s future.
Key Takeaway: While breast milk is remarkably resilient and maintains adequate macronutrient content even when maternal diet is suboptimal, the quality of micronutrients, fatty acid profiles, immune-modulating compounds, and flavor molecules directly reflects a mother’s intake. Optimizing diet empowers a child’s neurological development, allergy resistance, and metabolic programming, making postpartum nutrition a powerful lever for lifelong health.
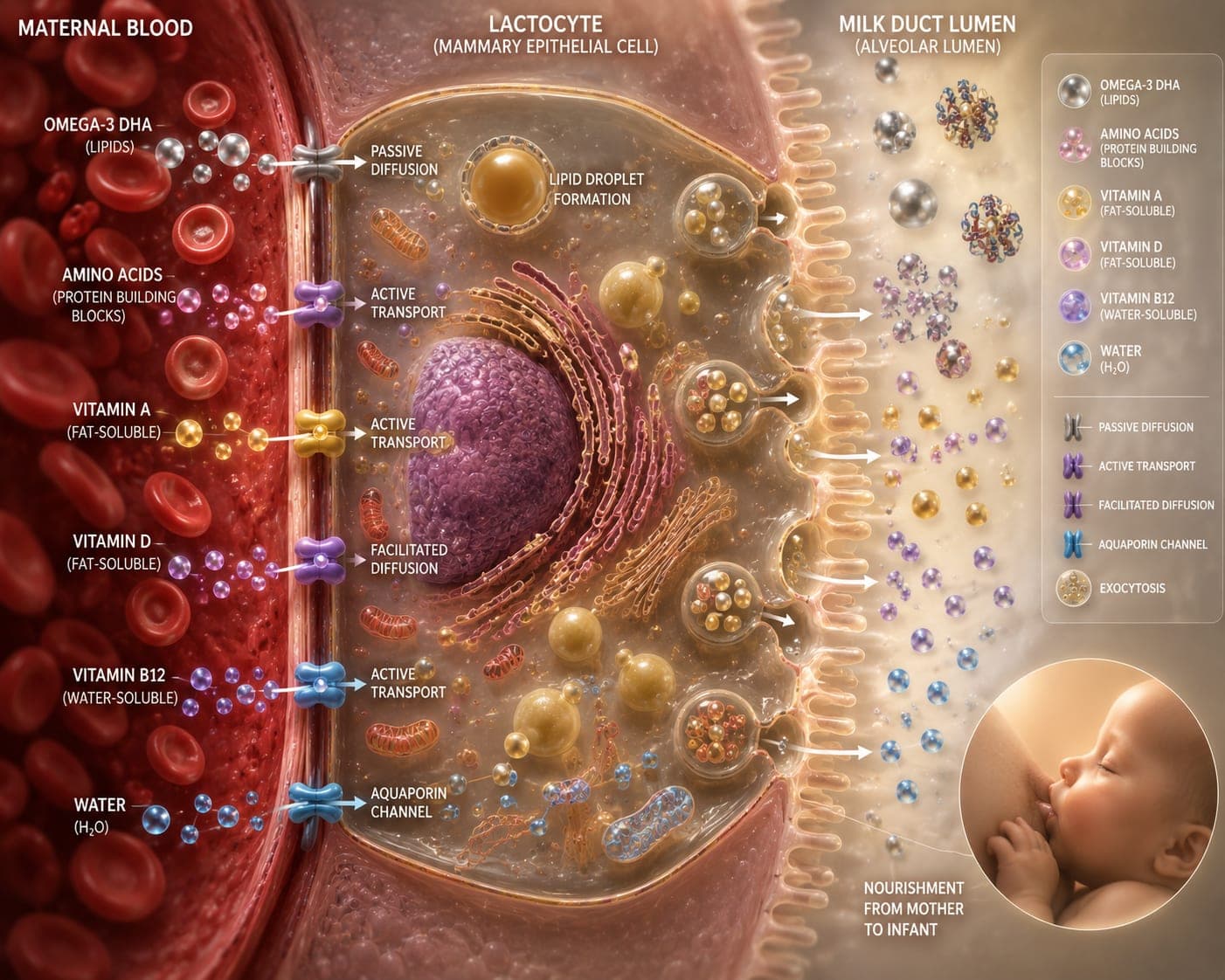
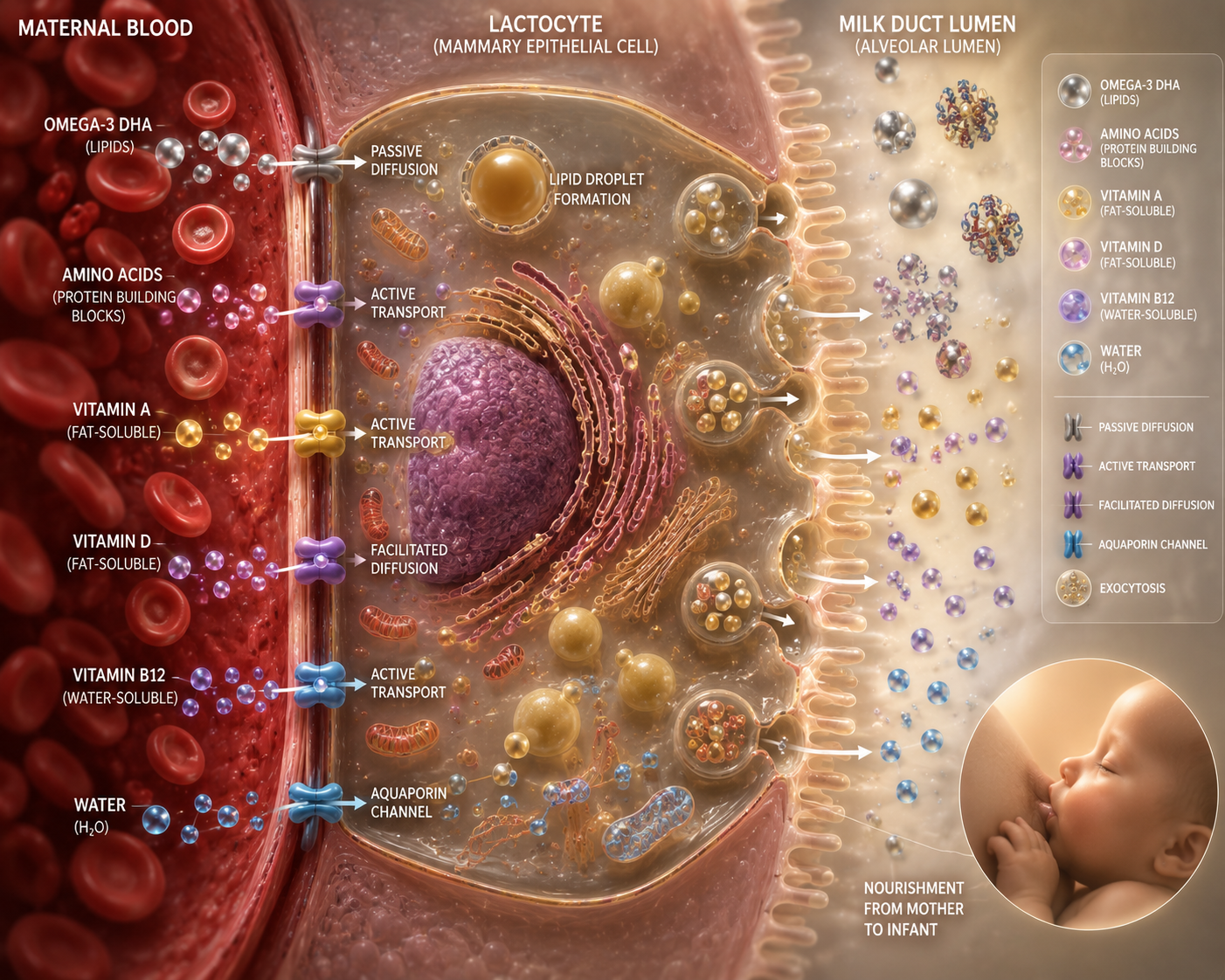
The Biological Mechanism: From Mother’s Plate to Mammary Gland
To appreciate how foods affect breast milk, one must understand the lactocyte—the milk-secreting cell lining the mammary alveoli. Nutrients arrive via maternal blood and cross the lactocyte through five major pathways: transcellular diffusion, facilitated transport, active transport, paracellular leakage, and transcytosis. Fat-soluble vitamins, fatty acids, and many immune factors rely on active transport or packaging into milk fat globules. Water-soluble vitamins like B12 and folate are tightly regulated by active carrier proteins. This sophisticated gatekeeping explains why some dietary components rapidly shift milk composition while others remain constant. However, a chronically depleted maternal diet eventually compromises both mother and infant, as the gland sacrifices maternal stores to maintain milk levels, progressively draining the mother’s own muscle, bone, and brain nutrient reserves.
Key Dietary Components That Directly Impact Breast Milk
Protein: Quantity, Quality, and Bioactive Peptides
Total protein content in breast milk is remarkably stable around 0.9–1.2 g/dL and does not fluctuate dramatically with short-term maternal intake. Yet chronic protein-energy malnutrition does lower milk protein output. More importantly, the immunomodulatory protein profile—lactoferrin, secretory IgA, lysozyme—is enhanced by a well-nourished mother. Additionally, dietary sources of specific amino acids influence milk taurine and carnitine levels, both critical for neonatal brain and heart development. Nursing mothers should prioritize 1.5–1.7 g of high-quality protein per kg of body weight daily from pastured eggs, grass-fed whey, collagen peptides, wild salmon, and legumes. This not only supports milk protein quality but spares maternal lean mass during the catabolic demands of lactation.
DHA: The Omega-3 That Builds a Smarter Brain
The fatty acid profile of breast milk is the single most diet-responsive macronutrient fraction. Docosahexaenoic acid (DHA), a long-chain omega-3, concentrates in the infant’s cerebral cortex and retinal photoreceptors, with accretion peaking in the third trimester and continuing through the first two years of breastfeeding. Milk DHA levels in Western mothers typically fall between 0.1–0.4% of total fatty acids, but studies show that consuming 200–300 mg of DHA daily can elevate breast milk DHA to 0.8–1.0%, a range associated with improved infant visual acuity and cognitive processing speed at 12 months. Fatty cold-water fish (wild salmon, sardines, herring) two to three times weekly or a molecularly distilled algae oil supplement is the most reliable strategy. Vegan mothers benefit particularly from algae-derived DHA, which bypasses the inefficient conversion from alpha-linolenic acid found in flax and chia.
Vitamins: The Fat-Soluble Versus Water-Soluble Divide
The transfer of vitamins into breast milk depends heavily on solubility and maternal status. Fat-soluble vitamins A and K are actively transported in a tightly regulated manner; maternal supplementation improves milk levels only when stores are deficient. Conversely, water-soluble vitamins like B-complex (B12, riboflavin, niacin, folate) and vitamin C rapidly reflect maternal intake. A diet rich in dark leafy greens, citrus, organ meats, and nutritional yeast ensures adequate B12 and folate, preventing megaloblastic anemia in exclusively breastfed infants. Vitamin D is a critical exception: breast milk is inherently low in vitamin D, regardless of maternal intake, which is why the American Academy of Pediatrics recommends direct infant supplementation of 400 IU daily from birth. Nursing mothers should still maintain their own vitamin D status above 40 ng/mL for personal bone health and immune resilience.
Hydration: The Misunderstood Driver of Milk Supply
Contrary to popular belief, forcing excessive fluids does not directly increase milk volume; milk synthesis is driven by infant demand and prolactin, not by overhydration. However, chronic dehydration does reduce milk output and thickens milk viscosity. The mammary gland is a remarkably privileged tissue that will pull water from the maternal compartment to maintain production, but at the cost of maternal dry skin, headaches, and fatigue. The practical guideline: drink to thirst, aiming for approximately 2.5–3.5 liters of total water daily, with herbal teas, bone broth, and electrolyte-rich coconut water contributing to hydration while delivering trace minerals. Overhydration can actually dilute sodium concentrations and suppress the osmotic gradient needed for efficient milk ejection, a little-known biological nuance.
| Nutrient | Maternal Target Daily | Effect on Breast Milk & Infant | Top Food Sources |
|---|---|---|---|
| DHA | 200–300 mg | Enhances cortical synapses, visual development; milk level triples with consistent intake | Wild salmon, sardines, algae oil |
| Choline | 550 mg | Directly secreted into milk; fuels hippocampal memory center formation | Egg yolks, liver, sunflower lecithin |
| Vitamin B12 | 2.8 mcg | Milk levels drop within days of low intake; prevents infant neuroregression | Clams, grass-fed beef, nutritional yeast |
| Vitamin A | 1300 mcg RAE | Milk content adequate unless maternal deficiency; essential for infant immune organs | Beef liver, sweet potato, carrots |
| Iodine | 290 mcg | Concentrated 20–50 times in milk vs. blood; critical for thyroid hormone-driven brain myelination | Seaweed, cod, iodized salt |
| Fluids | 2.5–3.5 L total | Prevents dehydration-related supply dips; supports milk ejection reflex | Water, bone broth, coconut water |
Pro Tip: A simple “lactation smoothie” combining frozen wild blueberries (anthocyanins for infant endothelium), raw almonds (vitamin E), a scoop of grass-fed collagen (glycine for milk synthesis and maternal skin repair), and flaxseed (fiber for satiety) delivers a synergistic nutrient punch that upgrades milk quality and sustains energy through cluster-feeding sessions.
Modern Insights: Timing, Gut-Axis Communication, and Flavor Programming
Emerging research reveals that breast milk is not just a nutrient depot but a conduit for maternal metabolic signals and sensory education. The entero-mammary axis is a gut-breast immunological highway: a mother’s gut microbiota influences the types of beneficial bacteria and oligosaccharides that appear in her milk, training the infant’s immune system to distinguish friend from foe. Consuming fermented foods like kefir, kimchi, and unsweetened yogurt while minimizing emulsifiers and artificial sweeteners enriches milk with immune-tolerizing microbes. Additionally, volatile flavor compounds from garlic, vanilla, mint, and cruciferous vegetables flavor amniotic fluid and breast milk, increasing an infant’s later acceptance of those foods during weaning. This is dietary imprinting—the earliest opportunity to shape a child’s palate toward nutrient-dense choices.
Common Myths vs. Facts
- Myth: “Drinking cow’s milk increases breast milk supply.”
Fact: No single food mechanically boosts supply. Milk production is demand-driven; galactagogues like fenugreek or goat’s rue may modulate prolactin receptors but work only in combination with frequent and effective milk removal. Dairy is not necessary and can sometimes trigger infant cow’s milk protein intolerance through mucosal transfer of bovine antigens. - Myth: “You need to avoid all spicy and gas-producing foods to prevent infant colic.”
Fact: Most infants tolerate maternal diet without issue. Only a small subset reacts to specific proteins (dairy, soy, egg). Reflux and fussiness are often due to oversupply, foremilk-hindmilk imbalance, or immature nervous system, not maternal broccoli consumption. Eliminating whole food groups without cause risks nutrient deficiencies. - Myth: “Alcohol helps with let-down and must be completely avoided.”
Fact: Alcohol inhibits oxytocin release and actually reduces milk ejection and total intake by the infant. Occasional, strategic consumption—one standard drink, waited out for 2+ hours per drink before nursing—is considered compatible with breastfeeding by the American Academy of Pediatrics, but zero alcohol remains the safest choice. - Myth: “If I don’t eat perfectly, my milk is unhealthy.”
Fact: The mammary gland is powerfully buffered. Even on a flawed diet, milk will sustain normal growth for a period. The risk is to the mother—her body will mobilize bone calcium, muscle amino acids, and liver stores to prioritize the infant. Feeding yourself well preserves your own long-term health while optimizing, not just safeguarding, the infant.
Frequently Asked Questions
Which specific foods are most likely to cause fussiness or allergies in my breastfed baby?
The most common dietary triggers transferred via breast milk are intact cow’s milk protein, followed by soy, egg, and wheat. Signs include mucousy, blood-flecked stools, severe eczema, or non-stop colic. If suspected, a 2–4 week elimination trial under a registered dietitian’s guidance can confirm sensitivity. It is critical not to self-diagnose and restrict multiple foods unnecessarily.
How quickly does my diet change breast milk composition?
Water-soluble vitamin and some fatty acid levels can shift within 4–8 hours of a single meal. DHA levels respond over days to weeks. Fat-soluble vitamin stores and total macronutrient ratios shift more slowly. This rapid adaptability means each feeding is a fresh opportunity to influence infant neurochemistry and metabolism.
Do I need to take a specific postnatal or lactation supplement?
Yes. A high-quality postnatal multivitamin should cover vitamin D, iodine, B12, methylfolate, and zinc. On top of that, supplementing 200–300 mg DHA from algae or fish oil is essential unless you eat fatty fish multiple times weekly. Many women also benefit from continued choline and magnesium, as lactation demands are even higher than pregnancy for several nutrients.
Can my vegetarian or vegan diet support healthy breast milk?
Absolutely, with meticulous planning. The primary risks are B12 deficiency (which can cause severe infant neuroregression), insufficient DHA, low iron, and marginal iodine. A well-formulated plant-based diet coupled with algae DHA, methylcobalamin (B12), and iodine from kelp or supplements produces milk fully compatible with infant growth. Regular blood monitoring of B12, iron, and vitamin D is non-negotiable.
How does exercise and maternal fitness affect breast milk?
Moderate exercise does not harm milk quality and may increase antioxidant levels. Vigorous maximal-intensity training can transiently elevate lactic acid in milk for up to 90 minutes post-exercise, potentially altering taste; some infants may briefly fuss. Pumping or nursing just before high-intensity sessions and staying well hydrated solves this. Exercise also supports prolactin receptor sensitivity and maternal mental health, indirectly benefiting breastfeeding success.
Conclusion: Your Postpartum Diet as a Legacy Investment
The composition of breast milk is a conversation between your body and your baby’s developing physiology. Every meal provides not only calories but information—coding for optimal brain architecture, metabolic set points, and immune tolerance. The focus keyword “foods that affect breast milk” encapsulates a truth that empowers: you are not just feeding hunger; you are molding a future. Prioritize high-DHA seafood, deeply colored vegetables, complete proteins, and adequate hydration. Reject the noise of unfounded restrictions. If you need a personalized lactation nutrition plan or fitness guidance to safely rebuild strength while protecting supply, our elite team of postpartum fitness coaches and sports nutrition experts is ready to create your protocol. Download our free “Lactation Optimization Guide” today and step into the most scientifically informed motherhood possible.
Medical & Health Disclaimer
The content provided in this article is for educational and informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician, lactation consultant, or another qualified health provider with any questions regarding your health or your infant’s health. Never disregard professional medical advice because of something you have read here.
Scientific References
- Koletzko B, Cetin I, Brenna JT, et al. Dietary fat intakes for pregnant and lactating women. Br J Nutr. 2007;98(5):873–877.
- Innis SM. Impact of maternal diet on human milk composition and neurological development of infants. Am J Clin Nutr. 2014;99(3):734S–741S.
- Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. 2013;60(1):49–74.
- Mennella JA, Jagnow CP, Beauchamp GK. Prenatal and postnatal flavor learning by human infants. Pediatrics. 2001;107(6):E88.
- Bravi F, Wiens F, Decarli A, Dal Pont A, Agostoni C, Ferraroni M. Impact of maternal nutrition on breast-milk composition: a systematic review. Am J Clin Nutr. 2016;104(3):646–662.
- Dror DK, Allen LH. Overview of nutrients in human milk. Adv Nutr. 2018;9(suppl_1):278S–294S.
- Patel S, Alvarez-Dorta D, Gao Y, et al. The entero-mammary pathway and mother-to-infant bacterial transmission. Cell Host Microbe. 2021;29(7):1089–1101.
Share


